We believe that safeguarding health in medical facilities starts with the fundamentals, and getting those fundamentals right every single time is what separates professional clinic cleaning sydney providers from general commercial cleaners. Our team has developed a set of necessary practices through years of working in GP clinics, specialist centres, dental surgeries, and day hospitals across Sydney. These are the tips and protocols that form the backbone of every medical cleaning services contract we deliver, and we share them here because we think every facility manager should understand what to expect from their cleaning provider.
PPE hierarchy in medical cleaning showing high medium and low risk equipment requirements with donning and doffing order for infection control
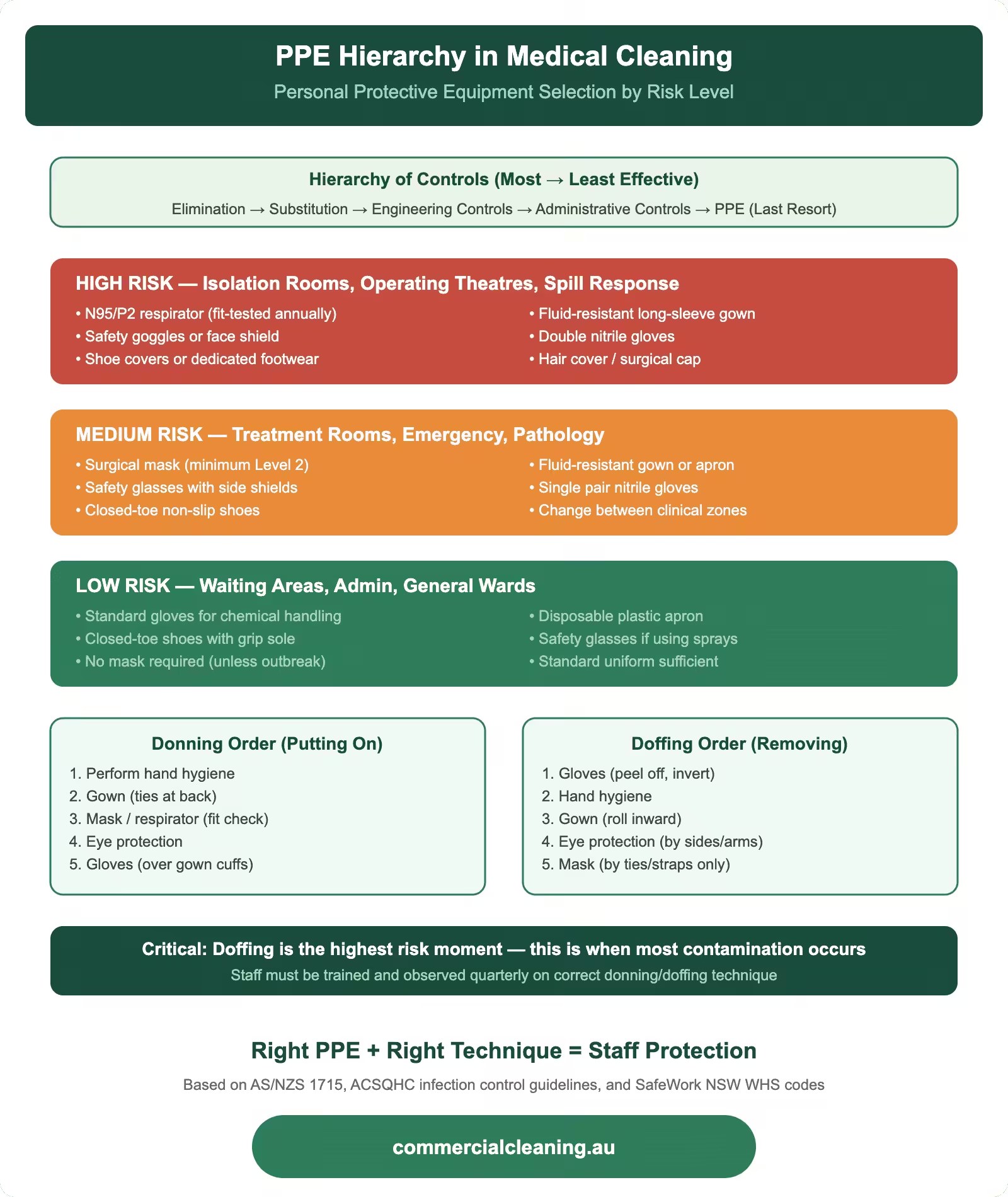
Personal Protective Equipment Hierarchy in Medical Cleaning
We enforce a strict PPE hierarchy across our medical cleaning operations that goes well beyond the basic gloves-and-apron approach many cleaning companies take. Our minimum standard for routine medical cleaning includes disposable nitrile gloves, a fluid-resistant disposable apron, and closed-toe slip-resistant shoes. For higher-risk tasks including biohazard spill response, isolation room cleaning, and clinical waste handling, we add a P2 respirator mask and protective eyewear. Our team members carry a full PPE kit on their person at all times so they can escalate their protection level immediately if the situation requires it without returning to their cleaning trolley.
We replace gloves between every room and every task change, which means a single team member on a medical cleaning shift can go through 40 to 60 pairs of gloves in an evening. We treat glove changes as non-negotiable because reusing gloves between rooms transfers pathogens directly from one clinical space to another. Our hand hygiene protocol requires alcohol-based hand rub application immediately after removing gloves and before donning a fresh pair. We audit glove change compliance through observational audits and have maintained a compliance rate above 98 percent across our medical contracts for the past year.
We source our PPE through a single verified supplier to confirm consistent quality and sizing across all our teams. After an incident at a medical centre in Colyton where a batch of cheaper imported gloves tore during a biohazard cleanup, we moved to a premium nitrile glove that offers better puncture resistance and tactile sensitivity. The cost increase was marginal but the safety improvement was significant, and our staff reported greater confidence handling contaminated materials. We factor PPE costs into every medical cleaning quote so clients never see their cleaning quality compromised by cost-cutting on protective equipment.
High-touch surface identification and prioritised disinfection infographic showing contact frequency pathogen survival times and ATP benchmarks for commercial cleaning
High-Touch Surface Identification and Prioritised Disinfection
We map every high-touch surface in a medical facility during our initial site assessment and build a prioritised disinfection schedule around that map. Our definition of a high-touch surface is any point that is contacted by multiple people more than once per hour during operating hours. In a typical GP clinic, this includes the reception counter, EFTPOS terminal, sign-in screen, door handles on every consultation room, shared computer keyboards, examination table adjustment levers, blood pressure cuff controls, and bathroom tap handles. We label these surfaces on our cleaning maps with red dots so every team member can see exactly which surfaces need attention during their high-touch rounds.
We clean high-touch surfaces a minimum of four times per day during operating hours, and we add an extra round during peak patient periods. Our teams use pre-impregnated hospital-grade disinfectant wipes for high-touch rounds because they offer the fastest turnaround and verify consistent disinfectant concentration on every wipe. Each wipe is used on a single surface and then discarded to prevent cross-contamination. We trialled reusable microfibre cloths with spray disinfectant for high-touch rounds but found that the time required to fold, spray, and wipe was 40 percent longer than using pre-impregnated wipes, which made it impractical during busy clinic hours.
Our high-touch round protocol requires the team member to work in a consistent direction through the facility so no surface gets missed. We train them to start at the main entrance and follow a clockwise route through reception, waiting area, corridor, consultation rooms, treatment rooms, and bathrooms. This systematic approach eliminates the randomness that leads to missed surfaces. We tested our compliance by placing UV fluorescent markers on high-touch surfaces at a medical centre in St Clair and found that our systematic route achieved 100 percent surface coverage compared to 82 percent coverage when cleaners were allowed to work in their own preferred order.
Healthcare Cleaning Risk Zone Comparison
Zone
Risk Level
Frequency
Disinfectant Grade
PPE Required
Operating Theatre
Critical
Between every case
Hospital-grade TGA
Full gown, gloves, mask
Patient Ward
High
2× daily + discharge
Hospital-grade TGA
Gloves, apron
Waiting Room
Medium
3× daily
Commercial-grade
Gloves
Admin Office
Low
Daily
General purpose
Gloves
Bathroom/Amenities
High
4× daily minimum
Hospital-grade TGA
Gloves, apron, eyewear
Hand Hygiene and Ventilation Management
Healthcare Cleaning Risk Zone Comparison requires specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We support hand hygiene compliance in every medical facility we clean by ensuring dispensers are always full, always functioning, and always positioned at the point of need. Our restocking protocol checks every hand sanitiser and soap dispenser during each cleaning round and tops them up before they drop below 25 percent capacity. We have noticed that compliance drops sharply when dispensers are empty or difficult to operate, so we also report any malfunctioning units to facility management immediately and carry spare dispensers in our vehicle to install as temporary replacements while repairs are arranged. Our commitment to keeping hand hygiene infrastructure operational around the clock is one of the most impactful contributions we make to infection prevention.
Ventilation management directly impacts cleaning effectiveness and we take it seriously even though it sits outside our primary scope. We monitor air quality in procedure rooms using particulate counters and report any anomalies to the facility’s maintenance team. Our cleaning methods are designed to minimise airborne particle generation — we use damp dusting rather than dry dusting, HEPA-filtered vacuums rather than standard models, and we avoid sweeping with dry brooms in clinical areas. When we clean ventilation grilles and air conditioning return filters, we seal them in bags immediately on removal to prevent dislodged dust from entering the clinical environment.
We encountered a ventilation issue at a pathology collection centre in Erskine Park where our air quality readings showed elevated particulate counts in the specimen processing area despite thorough surface cleaning. We investigated and found that the facility’s fume cupboard extraction system, which should comply with AS 4736 for laboratory fume cupboards, had a blocked pre-filter that was allowing recirculated air to bypass the HEPA stage. We reported this to the facility manager who arranged immediate servicing, and the particulate counts returned to normal within 24 hours. This kind of proactive environmental awareness costs our client nothing extra but can prevent serious contamination events.
Waste Management and Biohazard Containment
Waste Management and Biohazard Containment addresses specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We manage clinical waste streams in every medical facility we service using a strict colour-coded segregation system. Yellow bags and containers hold clinical waste including contaminated dressings, single-use procedure items, and materials that have come into contact with blood or body fluids. Purple containers hold cytotoxic waste from chemotherapy or oncology treatment areas. Grey or clear bags hold general non-clinical waste. We check every waste container during each cleaning round and replace clinical waste bags when they reach the three-quarter fill mark to prevent overfilling that creates handling hazards for our staff and the facility’s clinical team.
Our biohazard containment response follows a standardised protocol that every medical cleaning team member is trained and assessed on annually. When a blood or body fluid spill occurs, our team contains the area, applies granular absorbent, allows the specified contact time, collects the absorbed material into a clinical waste bag, and then disinfects the underlying surface with a chlorine-based solution at 10,000 parts per million. We document every biohazard incident on a dedicated form that records the time, location, type of material, volume estimate, cleaning agent used, and the name of the team member who responded. These records are retained for seven years and are available to the facility for audit and accreditation purposes.
We spend approximately $1,870 per year on specialised biohazard response training and equipment across our medical cleaning division, covering spill kits, PPE, training materials, and competency assessment resources. We consider this a non-negotiable investment because improperly managed biohazard spills represent one of the highest risk scenarios in medical facility cleaning. Our teams carry dedicated spill kits in sealed yellow containers that are separate from their general cleaning supplies, and we replace any kit that has been opened or used within 24 hours to make sure every team always has a complete kit available.
Training, Competency Assessment, and Continuous Improvement
Training, Competency Assessment, and Continuous Improvement targets specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We invest heavily in training our medical cleaning staff because the consequences of inadequate training in a healthcare environment are far more serious than in any other commercial cleaning setting. Every new team member completes a 40-hour induction programme that covers infection control principles, Spaulding classification, chemical safety, PPE usage, biohazard response, clinical waste segregation, and hand hygiene. They then complete a supervised probation period of four weeks where they work alongside an experienced medical cleaning technician before being cleared to work independently. We do not shortcut this process regardless of how urgently a new team member is needed on site.
Our ongoing competency assessment programme runs on a monthly cycle. Each team member is observed by a supervisor during a routine shift, and their performance is scored against a standardised rubric covering fifteen skill areas. The rubric includes PPE donning and doffing, glove change compliance, cloth folding and usage technique, chemical dilution accuracy, cleaning sequence adherence, documentation completion, and biohazard response readiness. Any skill area scoring below 80 percent triggers a targeted retraining session within the following week, and the team member is re-assessed at the next monthly cycle. We maintain individual training records for every team member and make them available to our clients on request.
We also run quarterly infection control update sessions where we bring in current information about emerging pathogens, updated guidelines from bodies like the NHMRC and RACGP, and lessons learned from incidents across our contract portfolio. These sessions keep our teams current and engaged, and they provide a forum for frontline staff to share their own observations and suggestions. Some of our best process improvements have come from team members who noticed a problem during their daily work and raised it during these sessions. We encourage that culture of continuous improvement because our clients benefit directly from every incremental gain in cleaning quality. For guidance on infection control standards and cleaning protocols specific to medical facilities, we recommend exploring our next article in our medical cleaning series on infection control standards.
Frequently Asked Questions on Medical Facility Cleaning Essentials
What personal protective equipment is mandatory for healthcare cleaning staff? We require disposable nitrile gloves, fluid-resistant disposable aprons, and closed-toe slip-resistant shoes as the minimum for routine medical cleaning. For higher-risk tasks like biohazard response and isolation room cleaning, we add P2 respirator masks and protective eyewear. Gloves are changed between every room and task, and hand hygiene is performed immediately after glove removal and before donning a fresh pair.
How should colour-coded microfibre cloths be implemented to prevent cross-contamination? We assign specific colours to specific zones: blue for general clinical areas, red for bathrooms, green for kitchens and break rooms, and yellow for isolation and high-risk clinical zones. Each cloth is single-use within its designated zone and folded into quarters to provide eight clean faces. Cloths are bagged separately after use and thermally disinfected at temperatures above 70 degrees Celsius before reissue.
What surfaces require prioritised disinfection in medical facilities? We prioritise any surface contacted by multiple people more than once per hour, including reception counters, EFTPOS terminals, door handles, computer keyboards, examination table controls, blood pressure cuff holders, and bathroom tap handles. These high-touch surfaces are cleaned a minimum of four times daily during operating hours using hospital-grade disinfectant wipes.
How can healthcare staff and patients improve hand hygiene compliance? We support hand hygiene compliance by ensuring dispensers are always full, functional, and positioned at the point of need. We check every dispenser during each cleaning round and top them up before they drop below 25 percent capacity. Malfunctioning units are reported immediately and we carry spare dispensers to install as temporary replacements while repairs are arranged.
What role do ventilation systems play in infection prevention? Ventilation systems control airborne pathogen transmission and particle levels in clinical spaces. We monitor air quality in procedure rooms, use damp dusting and HEPA-filtered vacuums to minimise airborne particle generation, and clean ventilation grilles carefully to prevent dislodged dust from entering clinical areas. We report any air quality anomalies to the facility’s maintenance team for immediate investigation.
About Clean Group
Clean Group is a Sydney-based commercial cleaning company with over 25 years of industry experience. Founded by Suji Siv, our team of 50+ trained professionals services offices, warehouses, medical centres, schools, childcare facilities, retail stores, gyms, and strata properties across Sydney, Melbourne, and Brisbane.
We are active members of ISSA and the Building Service Contractors Association of Australia (BSCAA). Our operations align with ISO 9001 (Quality Management), ISO 14001 (Environmental Management), and ISO 45001 (Workplace Health and Safety) standards. We hold membership with the Green Building Council of Australia and use eco-friendly, TGA-registered cleaning products wherever possible.
Every Clean Group cleaner is police-checked, fully insured, and trained in safe work procedures under SafeWork NSW guidelines. We operate 7 days a week, including after-hours and weekend services, to minimise disruption to your business.
Hi, I'm Suji Siv, the founder, CEO, and Managing Director of Clean Group, bringing over 25 years of leadership and management experience to the company. As the driving force behind Clean Group’s growth, I oversee strategic planning, resource allocation, and operational excellence across all departments. I am deeply involved in team development and performance optimization through regular reviews and hands-on leadership.