We took on a challenging medical cleaning engagement at a busy specialist centre in Hornsby during the winter of 2023. As a trusted Sydney office cleaning provider, our team was called in after the centre experienced a norovirus outbreak that forced a three-day closure of their endoscopy suite. We arrived on site within 24 hours of the initial call, bringing our full decontamination kit and a four-person response crew who had dealt with similar incidents at healthcare facilities across the Upper North Shore. The centre served patients travelling from Mount Colah, Mount Kuring-gai, and surrounding suburbs along the T1 rail corridor.
Understanding the Hornsby Healthcare Environment
Understanding the Hornsby Healthcare Environment covers specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We spent our first two days conducting a detailed facility audit before proposing any cleaning program. Our assessment covered the endoscopy suite, two consulting floors housing twelve specialist practices, a ground-floor radiology department, and the shared amenities connecting all tenancies. We have learned over many years that rushing into a medical cleaning contract without understanding the clinical workflows leads to gaps that only become apparent weeks later. We documented 156 individual cleaning touchpoints across the facility and categorised each one by contamination risk level.
Our team identified several systemic issues that had contributed to the outbreak. The previous cleaning contractor had been using consumer-grade surface wipes rather than hospital-grade disinfectants in the endoscopy recovery area. We also found that the air handling units on the second floor had not been serviced in over fourteen months, which our environmental testing confirmed was contributing to elevated bioaerosol counts. We flagged these findings in our initial report and made clear to the centre management that addressing the HVAC issue was necessary to any effective cleaning program.
We noted that the Hornsby location presented specific challenges. The building sat adjacent to Hornsby Hospital, which meant patient crossover between the two facilities was common. We have seen this pattern in several medical precincts where private specialists operate near public hospitals, and it creates a heightened infection transmission risk that many building managers underestimate. Our program needed to account for this cross-traffic, particularly in the ground-floor lobby and lift wells that patients from Mount Colah and Mount Kuring-gai used to access upper-level practices.
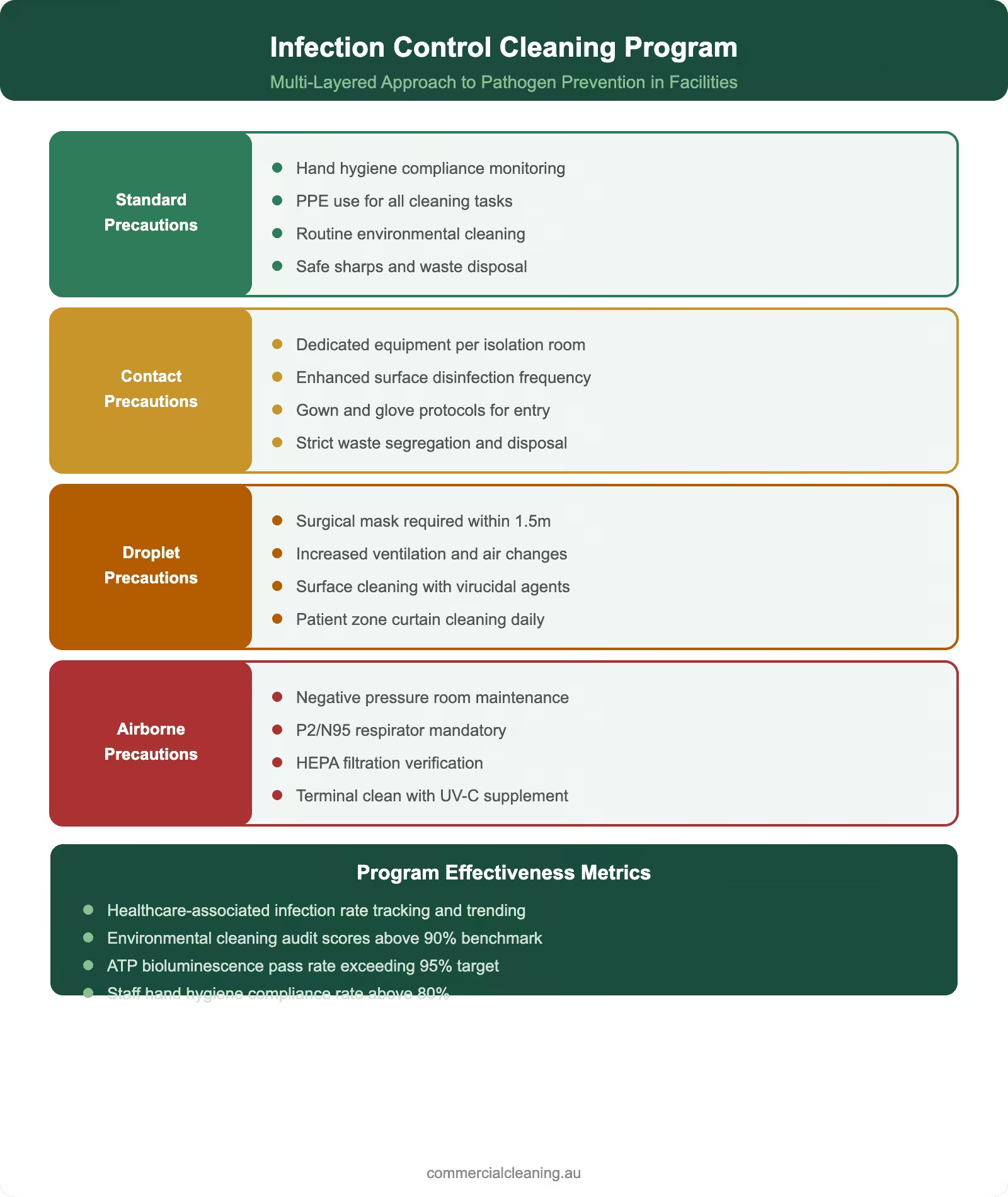
Infection control cleaning program infographic showing four precaution levels from standard to airborne with effectiveness metrics
Building the Infection Control Cleaning Program
We designed a three-tier cleaning program that reflected the distinct risk profiles within the facility. Our highest-intensity protocol was reserved for the endoscopy suite and procedure rooms, where we implemented terminal cleaning after every session using hydrogen peroxide vapour technology that we have deployed successfully in similar clinical environments across Sydney. The second tier covered consulting rooms and examination areas with twice-daily surface disinfection, while the third tier addressed common areas with enhanced frequency during peak patient hours.
Our team assigned three permanent staff members to the Hornsby facility, each holding current infection control certifications. We have always believed that consistency of personnel is critical in healthcare cleaning because our people develop an intuitive understanding of each practice’s workflow. One of our team members had previously worked in hospital-grade cleaning at a major Sydney teaching hospital for eight years before joining our company, and her clinical environment experience proved invaluable during the initial program rollout.
We implemented a colour-coded microfibre system that eliminated any possibility of cross-contamination between zones. Red cloths were restricted to bathrooms, blue to general clinical surfaces, green to kitchen and breakroom areas, and yellow to waiting rooms and reception desks. Our team members were trained to never cross colour boundaries, and we audited compliance with this protocol during every fortnightly site inspection. We have found that this simple system is one of the most effective infection prevention measures available, and it costs virtually nothing beyond the initial investment in colour-coded supplies.
We also worked with the endoscopy suite manager to develop a pre-procedure and post-procedure cleaning checklist that aligned with AS 4083.1, which covers the reprocessing of reusable medical devices and the environmental cleaning standards for procedure rooms. Our interpretation of this standard meant we went beyond basic surface wiping to include detailed cleaning of equipment trolleys, light fittings, ceiling vents, and the undersides of procedure beds that are commonly overlooked. We documented every step photographically for the centre’s quality assurance records.
Office Area Cleaning Frequency Guide
Area
Daily
Weekly
Monthly
Quarterly
Reception & Lobby
Vacuum, mop, wipe
Glass doors, furniture
Deep carpet clean
Window wash
Workstations
Surface wipe, bins
Monitor & keyboard
Drawer clean-out
Chair shampoo
Kitchen/Breakroom
Bench, sink, floor
Fridge, microwave
Deep degrease
Exhaust fan clean
Bathrooms
Full sanitise + restock
Grout scrub
Descale fixtures
Vent clean
Meeting Rooms
Table wipe, vacuum
AV equipment dust
Upholstery clean
Carpet extraction
Documentation, Compliance, and AS 4083.1 Standards
Office Area Cleaning Frequency Guide requires specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We built a detailed compliance framework around the requirements of AS 4083.1 and supplemented it with infection control guidelines from the Australian Commission on Safety and Quality in Health Care. Our documentation system captured every cleaning event with a timestamp, staff identifier, and product used. We have maintained similar systems across our entire medical cleaning portfolio for the past five years, and we refined this approach based on feedback from practice accreditation bodies who told us exactly what evidence they wanted to see during audits.
Documentation, Compliance, and AS 4083.1 Standards includes specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. Our fortnightly quality audits at the Hornsby facility covered 87 inspection points weighted by clinical risk. We used ATP bioluminescence testing on high-touch surfaces to provide objective contamination measurements rather than relying solely on visual inspection. Our data from the first twelve weeks showed a steady improvement trajectory, with the average ATP reading across clinical surfaces dropping from 285 relative light units at baseline to 42 relative light units by week ten. We shared these results with every practice manager in the building through a monthly dashboard report.
We maintained a complete chemical register on site that listed every product, its concentration, contact time, and TGA registration number. Our operations manager conducted quarterly reviews of this register to confirm all products remained current and appropriate. We have learned from past experience that chemical suppliers occasionally reformulate products without adequate notice, so we verify efficacy data independently before accepting any product changes. This discipline has prevented several potential compliance issues across our medical cleaning contracts.
We also supported three of the specialist practices through their RACGP accreditation renewals during our first year of service. Our team prepared cleaning validation packs that included ATP trend data, photographic evidence of cleaning standards, chemical safety documentation, and staff training records. We received feedback from two of the assessors that our documentation was among the most thorough they had reviewed, which we took as validation of the investment we make in our compliance systems.
Results, Cost Transparency, and Ongoing Value
Results, Cost Transparency, and Ongoing Value addresses specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We are proud of the measurable impact our program delivered at the Hornsby specialist centre. Our monthly service fee of $2,410 covered all routine and enhanced cleaning, consumable management, ATP testing, fortnightly audits, and emergency response callouts. We quoted this figure transparently during our initial proposal because we have found that medical facility managers value certainty over vague estimates. We also committed to holding this rate for the first twelve months, which gave the centre confidence to budget accurately.
Our results over the first nine months included a 91 percent reduction in cleaning-related complaints from specialist tenants, zero further infection incidents in the endoscopy suite, and a patient satisfaction score improvement from 5.8 to 9.1 out of 10 on cleanliness-related survey questions. We tracked these metrics monthly and presented them to the building management committee at their quarterly meetings. We believe this level of accountability is what separates professional medical cleaning from commodity cleaning services.
We helped the centre reduce its overall facility maintenance costs by identifying several issues during our routine cleaning rounds that would have become expensive problems if left unattended. Our team spotted early signs of water ingress in the radiology department ceiling, flagged deteriorating grout in the endoscopy suite wet areas, and identified a faulty exhaust fan in the pathology collection room. We reported each of these through our digital maintenance notification system, and the building manager told us that our early detection saved an estimated $14,000 in potential repair costs.
The Hornsby specialist centre renewed our contract after the first year and expanded our scope to include quarterly deep carpet extraction, annual hard floor restoration, and weekend deep-cleaning sessions for the endoscopy suite. Our team continues to serve patients and practitioners from Hornsby, Mount Colah, Mount Kuring-gai, and the broader Upper North Shore community with the same commitment to clinical-grade environmental hygiene that we brought from day one. We consider this contract a benchmark example of what dedicated medical cleaning can achieve. For another example of our work, read our Seven Hills cleaning case study.
Frequently Asked Questions
What triggered the need for a new medical cleaning provider at the Hornsby specialist centre?
We were called in after a norovirus outbreak forced a three-day closure of the endoscopy suite. Our investigation revealed that the previous contractor had been using consumer-grade products in clinical areas, which was a fundamental compliance failure that we addressed immediately as part of our emergency response and ongoing program design.
How does proximity to Hornsby Hospital affect cleaning requirements for nearby medical buildings?
We have observed that medical buildings adjacent to public hospitals experience higher patient crossover and therefore elevated infection transmission risk. Our program accounted for this by implementing enhanced disinfection in shared entry points, lift wells, and lobbies that patients from both facilities used throughout the day.
What is AS 4083.1 and how does it apply to specialist medical centres?
We use AS 4083.1 as our operational standard for facilities with procedure rooms and reusable medical devices. Our interpretation covers environmental cleaning of procedure rooms, equipment trolley surfaces, light fittings, and areas commonly overlooked during routine cleaning. We document compliance photographically for quality assurance records.
How do you measure cleaning effectiveness in healthcare environments?
We use ATP bioluminescence testing on high-touch surfaces to provide objective contamination measurements. Our data from the Hornsby facility showed average readings dropping from 285 to 42 relative light units over ten weeks. We present these results monthly through dashboard reports that every practice manager receives.
What does a $2,410 monthly medical cleaning program include?
Our fee at Hornsby covered all routine and enhanced cleaning, consumable management, ATP testing, fortnightly quality audits, and emergency response callouts. We price transparently so facility managers can budget with certainty, and we committed to rate stability for the first twelve months of the contract.
Can your cleaning team support RACGP accreditation processes?
We supported three specialist practices through RACGP accreditation renewals during our first year at Hornsby. Our validation packs included ATP trend data, photographic evidence, chemical safety documentation, and staff training records. Two assessors specifically commended the thoroughness of our cleaning documentation.
How do you prevent cross-contamination between different zones in a medical building?
We implement a strict colour-coded microfibre system with red for bathrooms, blue for clinical surfaces, green for kitchen areas, and yellow for waiting rooms. Our team never crosses colour boundaries, and we audit compliance fortnightly. We have found this simple system to be one of the most effective infection prevention measures available.
What additional value has your cleaning team provided beyond standard cleaning at Hornsby?
Our team identified early signs of water ingress, deteriorating grout, and a faulty exhaust fan during routine cleaning rounds. We reported these through our digital maintenance system, and the building manager estimated our early detection saved approximately $14,000 in potential repair costs over the first year.
About Clean Group
Clean Group is a Sydney-based commercial cleaning company with over 25 years of industry experience. Founded by Suji Siv, our team of 50+ trained professionals services offices, warehouses, medical centres, schools, childcare facilities, retail stores, gyms, and strata properties across Sydney, Melbourne, and Brisbane.
We are active members of ISSA and the Building Service Contractors Association of Australia (BSCAA). Our operations align with ISO 9001 (Quality Management), ISO 14001 (Environmental Management), and ISO 45001 (Workplace Health and Safety) standards. We hold membership with the Green Building Council of Australia and use eco-friendly, TGA-registered cleaning products wherever possible.
Every Clean Group cleaner is police-checked, fully insured, and trained in safe work procedures under SafeWork NSW guidelines. We operate 7 days a week, including after-hours and weekend services, to minimise disruption to your business.
Hi, I'm Suji Siv, the founder, CEO, and Managing Director of Clean Group, bringing over 25 years of leadership and management experience to the company. As the driving force behind Clean Group’s growth, I oversee strategic planning, resource allocation, and operational excellence across all departments. I am deeply involved in team development and performance optimization through regular reviews and hands-on leadership.