We have applied the Spaulding classification system to surface medical cleaning sydney decisions in healthcare facilities for over a decade, and we consider it the single most important framework any cleaning provider must understand before touching a surface in a clinical environment. Our team uses this classification every day across our healthcare contracts because it eliminates guesswork and ensures that every surface receives the appropriate level of disinfection based on its infection transmission risk. As medical centre cleaning specialists working across Sydney, we have seen first-hand how facilities that embrace Spaulding classification achieve consistently better infection control outcomes than those relying on a one-size-fits-all cleaning approach. We have classified surfaces in medical centres across Hurstville, Beverly Hills, and Penshurst, and the process reveals misclassification issues in virtually every facility we assess for the first time.
Our experience tells us that the Spaulding classification is not just an academic exercise — it has direct, measurable consequences for patient safety and cleaning resource allocation. We have encountered facilities where critical surfaces were cleaned with products appropriate only for non-critical items, creating genuine infection risks that went unrecognised until our assessment highlighted the gaps. We have also seen the opposite — facilities wasting money and damaging surfaces by applying aggressive high-level disinfection to non-critical items that only required low-level treatment. We believe that proper Spaulding classification is the foundation upon which every other cleaning decision should rest, and we build every healthcare cleaning programme around this principle.
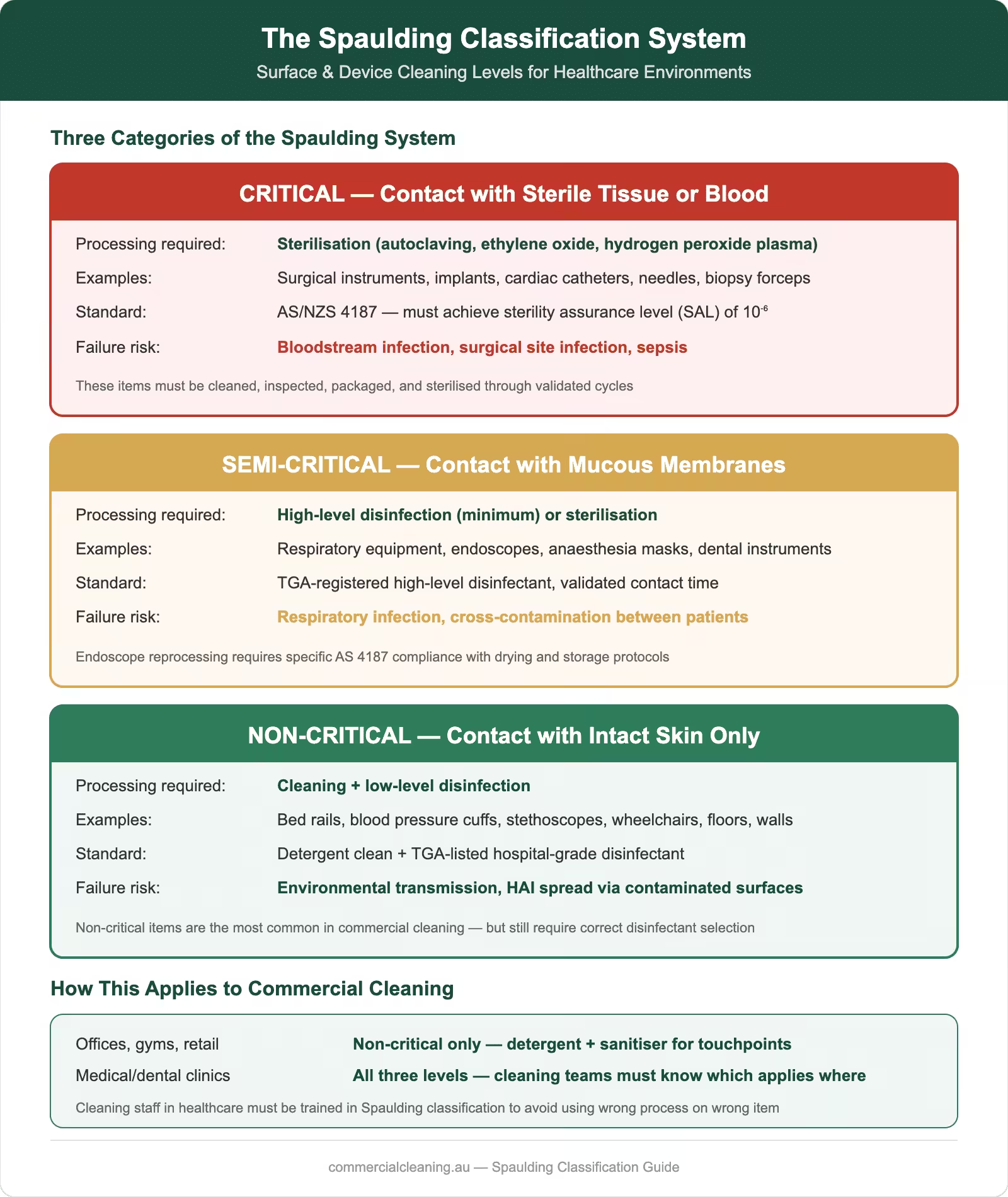
Spaulding classification system infographic showing critical, semi-critical, and non-critical categories with processing requirements, examples, and standards for healthcare cleaning
What Is the Spaulding Classification System
We explain the Spaulding classification to every client we work with because understanding the framework helps them appreciate why we make different cleaning decisions for different surfaces. The system was developed by Dr Earle Spaulding in 1968 and categorises medical items and environmental surfaces into three risk levels based on the degree of infection risk associated with their use. Critical items contact sterile tissue or the vascular system and require sterilisation. Semi-critical items contact mucous membranes or non-intact skin and require high-level disinfection at minimum. Non-critical items contact only intact skin and require low to intermediate-level disinfection depending on the contamination context.
Our teams apply this classification both to reusable medical devices — which is its original purpose — but to all environmental surfaces within the healthcare facility. We have found this extended application invaluable because it provides a consistent decision framework that our operatives can apply to any surface they encounter. We classify examination tables as semi-critical when they are used for procedures involving mucous membrane contact, treatment room benchtops as semi-critical when instruments are placed directly on them, and waiting room chairs as non-critical because they contact only clothed intact skin. We document every classification decision in our site-specific cleaning manual so that any operative can verify the correct treatment for any surface.
Critical Items: Sterilisation Requirements
We do not directly handle critical item reprocessing as environmental cleaning providers, but we understand the critical category thoroughly because it informs how we manage the surfaces and environments where these items are stored, prepared, and used. Critical items include surgical instruments, implants, cardiac catheters, and any device that penetrates sterile tissue or enters the vascular system. These items require sterilisation — the complete elimination of all forms of microbial life including bacterial spores — and this is achieved through autoclaving, ethylene oxide gas exposure, or hydrogen peroxide plasma sterilisation in dedicated reprocessing departments.
Our role with critical items focuses on maintaining the environmental conditions that support sterile storage and handling. We clean and disinfect sterile storage areas, instrument preparation rooms, and the surfaces surrounding autoclave and steriliser equipment using methods that prevent environmental contamination from compromising the sterility of processed instruments. We have worked with sterilisation departments in Hurstville medical centres where our environmental cleaning schedule was specifically designed to complement the facility’s instrument reprocessing workflow, ensuring that bench surfaces were disinfected before clean instruments were placed on them and that air quality was maintained through HEPA-filtered ventilation system cleaning.
We focus significant attention on semi-critical classification because this category generates the most confusion and the most classification errors in the facilities we assess. Semi-critical items contact mucous membranes or non-intact skin but do not penetrate sterile tissue — examples include respiratory therapy equipment, anaesthesia breathing circuits, endoscopes, and laryngoscope blades. These items require high-level disinfection that eliminates all microorganisms except high numbers of bacterial spores. We align our surface disinfection practices in rooms where semi-critical items are used with the principles established in AS 2773, which governs ultrasonic cleaners used in healthcare instrument reprocessing and establishes validation standards we apply to our surface disinfection verification processes.
Our environmental cleaning protocols for rooms containing semi-critical items use intermediate to high-level disinfection for all surfaces within the immediate use zone. We apply accelerated hydrogen peroxide to examination tables, headrests, and equipment surfaces in treatment rooms where respiratory assessments, wound care, or other mucous membrane contact procedures are performed. We have found that many facilities in Beverly Hills and Penshurst underestimate the number of semi-critical contact events that occur in general consultation rooms — activities like ear examinations with otoscopes, nasal swab collection, and oral cavity assessment all involve semi-critical contact, yet the room surfaces are often cleaned to non-critical standards.
We conduct semi-critical surface audits at every healthcare facility we service, and our findings consistently reveal surfaces that should be classified as semi-critical but are being treated as non-critical. Our most common finding is examination table surfaces in general practice rooms — these surfaces contact patient skin during examinations that may involve non-intact skin or mucous membranes, yet many facilities clean them with the same low-level quaternary ammonium products used in waiting rooms. We reclassify these surfaces during our assessment and upgrade the disinfection protocol accordingly, typically switching from a five-minute quat to an accelerated hydrogen peroxide product with proven intermediate-level efficacy.
Non-Critical Items: Low to Intermediate-Level Disinfection
We manage the largest volume of non-critical surfaces in our healthcare cleaning programmes because these surfaces make up the majority of the built environment in any medical facility. Non-critical items and surfaces contact only intact skin or no patient contact at all — examples include bed rails, bedside tables, blood pressure cuffs, stethoscope bodies, floors, walls, countertops in non-clinical areas, and furniture in waiting rooms and administrative offices. We apply low-level disinfection using TGA-registered quaternary ammonium compounds with demonstrated efficacy against vegetative bacteria, most viruses, and fungi.
We escalate non-critical surface disinfection to intermediate level in specific circumstances that our protocols define explicitly. When a non-critical surface is visibly contaminated with blood or body fluids, we apply intermediate-level disinfection regardless of its baseline Spaulding classification. When a facility is managing an outbreak of a multi-drug-resistant organism, we upgrade all non-critical surfaces in affected areas to intermediate-level treatment. We have implemented these escalation protocols across our Hurstville aged care contracts, and we find that having clear trigger criteria prevents both under-treatment during high-risk situations and unnecessary over-treatment during routine operations.
Misclassification: Common Mistakes and Prevention
We encounter Spaulding misclassification errors at virtually every new healthcare facility we assess, and we have identified the most common patterns that lead to inappropriate disinfection levels. The single most frequent error we see is classifying examination table surfaces as non-critical when they should be semi-critical — this occurs because staff focus on the table’s construction material rather than the nature of patient contact that occurs on its surface. We have found this error in over sixty percent of the general practice facilities we have assessed across Beverly Hills and Penshurst, and correcting it typically requires upgrading the disinfection product from a standard quaternary ammonium to accelerated hydrogen peroxide.
We also frequently encounter reverse misclassification, where facilities apply high-level disinfection to surfaces that only require low-level treatment. While this might seem harmless from an infection control perspective, it wastes money on expensive chemicals, damages surface materials through unnecessary chemical exposure, and creates occupational health risks for cleaning staff who are exposed to more aggressive products than the situation warrants. We calculated that one Hurstville medical centre was spending approximately $2,290 per year more than necessary on disinfection chemicals because their previous cleaning contractor applied semi-critical-level products to every surface in the building regardless of classification. Our Spaulding-based protocol reduced their chemical costs by that amount while actually improving disinfection outcomes in the areas that genuinely needed higher-level treatment.
We prevent misclassification through our colour-coded zone mapping system that assigns a visual classification indicator to every surface in the facility. Our maps use green for non-critical, amber for semi-critical, and red for critical-adjacent surfaces, and we laminate these maps for display in cleaning storage areas and on our operatives’ digital devices. We update our classifications whenever a room’s clinical function changes, and we conduct annual reclassification audits to confirm our maps remain accurate as facilities evolve their service offerings.
Spaulding Classification in Australian Regulatory Context
We position our Spaulding classification practices within the broader Australian regulatory framework because compliance requires understanding how the classification integrates with national standards and guidelines. The NHMRC Australian Guidelines for the Prevention and Control of Infection in Healthcare explicitly reference the Spaulding classification as the foundation for reprocessing and environmental cleaning decisions in Australian healthcare facilities. We also reference AS 2773, which governs ultrasonic cleaners used in healthcare reprocessing — this standard establishes validation principles for cleaning efficacy that we apply analogously to our environmental surface disinfection verification processes.
Our regulatory compliance approach ensures that every Spaulding classification decision we make is defensible against accreditation audit requirements. We document our classification rationale for every surface category, cross-reference our chemical selections against TGA registration data, and maintain evidence of operative training in classification-based cleaning procedures. We have supported multiple facilities through accreditation assessments across our Hurstville, Beverly Hills, and Penshurst contracts, and our Spaulding classification documentation has been specifically commended by assessors as evidence of systematic infection prevention governance.
Practical Decision-Making for Your Cleaning Team
We have developed a practical decision tool that our operatives use when they encounter a surface or item that is not covered by our existing classification maps. Our decision tree asks three questions: Does this item contact sterile tissue or the vascular system? If no, does it contact mucous membranes or non-intact skin? If no, does it contact only intact skin? These three questions reliably place any item or surface into the correct Spaulding category, and our operatives can apply them in under thirty seconds. We have found that giving our teams this analytical framework produces far better outcomes than simply providing lists of surfaces and their classifications, because lists cannot cover every situation while the decision framework can.
We reinforce practical classification skills through monthly scenario exercises where our team leaders present real-world situations and ask operatives to classify surfaces and select appropriate disinfection methods. Our scenarios are drawn from actual situations we have encountered across our portfolio — questions like whether a dental chair headrest requires semi-critical treatment when covered with a disposable barrier, or whether a GP examination couch requires reclassification when used for a skin biopsy procedure. We find that these discussions build genuine analytical capability that serves our teams far better than rote memorisation of classification lists.
Documentation and Compliance Verification
We document every aspect of our Spaulding classification system because undocumented classification decisions are unverifiable and therefore worthless from a compliance perspective. Our documentation package for each healthcare facility includes a complete surface classification register listing every surface category with its assigned Spaulding level and rationale, a chemical selection matrix mapping each classification level to approved disinfection products, and a verification schedule specifying the frequency and method of compliance testing for each surface category. We maintain these documents in our digital quality management system and make them available to facility managers through our secure client portal.
Our compliance verification programme uses ATP bioluminescence testing to objectively validate that our classification-based cleaning protocols are achieving the intended microbial reduction on each surface category. We test a random sample of surfaces from each Spaulding category at every facility on a monthly cycle, and we benchmark our results against published healthcare cleaning performance standards. Our current portfolio average shows ninety-two percent of tested surfaces meeting or exceeding the relevant benchmark for their classification level — a result we attribute directly to the precision that Spaulding-based cleaning brings compared to generic approaches. We share these results with our healthcare clients to continue exploring best practices, and we invite you to read our next guide on clinical waste handling.
Frequently Asked Questions
What is the Spaulding classification system?
We use the Spaulding classification as the foundation of every healthcare cleaning programme we design. Developed by Dr Earle Spaulding in 1968, it categorises surfaces and items into three risk levels — critical, semi-critical, and non-critical — based on infection transmission risk associated with patient contact. This determines the appropriate disinfection level for each surface in a healthcare facility.
How does Spaulding classification affect daily cleaning practices?
We assign specific disinfection products, contact times, and validation methods to each Spaulding category. Non-critical surfaces receive low-level quaternary ammonium disinfection. Semi-critical surfaces receive intermediate or high-level treatment with accelerated hydrogen peroxide. Critical-adjacent surfaces receive enhanced environmental controls. This targeted approach ensures every surface gets the right level of disinfection without waste or under-treatment.
What are the most common Spaulding misclassification errors?
We find that the most common error is classifying examination table surfaces as non-critical when patient contact with mucous membranes or non-intact skin makes them semi-critical. We have identified this error in over sixty percent of general practice facilities we assess. The reverse error — applying expensive high-level disinfection to genuinely non-critical surfaces — wastes money and damages surface materials unnecessarily.
What Australian Standards relate to Spaulding classification?
We reference AS 2773 for ultrasonic cleaner validation principles that we apply to surface disinfection verification, and the NHMRC Australian Guidelines for the Prevention and Control of Infection in Healthcare which explicitly references Spaulding classification as the foundation for reprocessing and environmental cleaning decisions in Australian healthcare facilities.
How do you train cleaning staff on Spaulding classification?
We train every healthcare cleaning operative using a three-question decision tree that reliably places any surface into the correct Spaulding category in under thirty seconds. We reinforce this with colour-coded zone maps, monthly scenario exercises using real-world situations from our portfolio, and practical observation assessments that test classification skills in live cleaning environments rather than classroom settings.
How much can proper Spaulding classification save on cleaning costs?
We have measured savings of approximately $2,290 per year in chemical costs alone at facilities that previously applied uniform high-level disinfection across all surfaces. Proper classification reduces chemical waste by matching product potency to actual risk, extends surface lifespan by avoiding unnecessary chemical exposure, and reduces occupational health risks for cleaning staff.
How often should Spaulding classifications be reviewed?
We conduct annual reclassification audits at every healthcare facility we service, with immediate reviews triggered whenever a room’s clinical function changes. We update our colour-coded zone maps and cleaning protocols immediately when reclassification occurs, and we communicate changes to all affected operatives within one business day.
Can Spaulding classification improve accreditation outcomes?
We have supported multiple facilities through accreditation assessments where our Spaulding classification documentation was specifically commended by assessors. Documented classification rationale, chemical selection matrices, and verification testing results demonstrate systematic infection prevention governance that accreditation auditors consistently recognise as best practice evidence.
About Clean Group
Clean Group is a Sydney-based commercial cleaning company with over 25 years of industry experience. Founded by Suji Siv, our team of 50+ trained professionals services offices, warehouses, medical centres, schools, childcare facilities, retail stores, gyms, and strata properties across Sydney, Melbourne, and Brisbane.
We are active members of ISSA and the Building Service Contractors Association of Australia (BSCAA). Our operations align with ISO 9001 (Quality Management), ISO 14001 (Environmental Management), and ISO 45001 (Workplace Health and Safety) standards. We hold membership with the Green Building Council of Australia and use eco-friendly, TGA-registered cleaning products wherever possible.
Every Clean Group cleaner is police-checked, fully insured, and trained in safe work procedures under SafeWork NSW guidelines. We operate 7 days a week, including after-hours and weekend services, to minimise disruption to your business.
Hi, I'm Suji Siv, the founder, CEO, and Managing Director of Clean Group, bringing over 25 years of leadership and management experience to the company. As the driving force behind Clean Group’s growth, I oversee strategic planning, resource allocation, and operational excellence across all departments. I am deeply involved in team development and performance optimization through regular reviews and hands-on leadership.