We have spent over fifteen years refining our approach to medical centre cleaning protocols, and we can say with confidence that the gap between facilities that follow structured procedures and those that improvise is enormous. Our team recently completed a full protocol overhaul for a busy multi-doctor practice in Epping, and the results reinforced what we have always believed — consistent, evidence-based cleaning is the single most effective barrier against healthcare-associated infections. As medical cleaners services providers working across Sydney, we see first-hand how proper protocols transform facility hygiene from reactive to preventive. We have cleaned hundreds of medical centres, and every one that embraces structured procedures sees measurable improvements in surface bioburden counts, staff confidence, and patient satisfaction scores.
Our experience tells us that medical centre cleaning demands a fundamentally different mindset from commercial or office cleaning. We are not just removing visible soil — we are systematically eliminating microbial reservoirs that pose direct risks to vulnerable patients. We have seen facilities in Eastwood where a single missed high-touch surface led to a cluster investigation, and we have watched practices in Marsfield achieve zero healthcare-associated infections over twelve consecutive months because they invested in proper cleaning protocols. This guide draws on everything we have learned across those engagements.
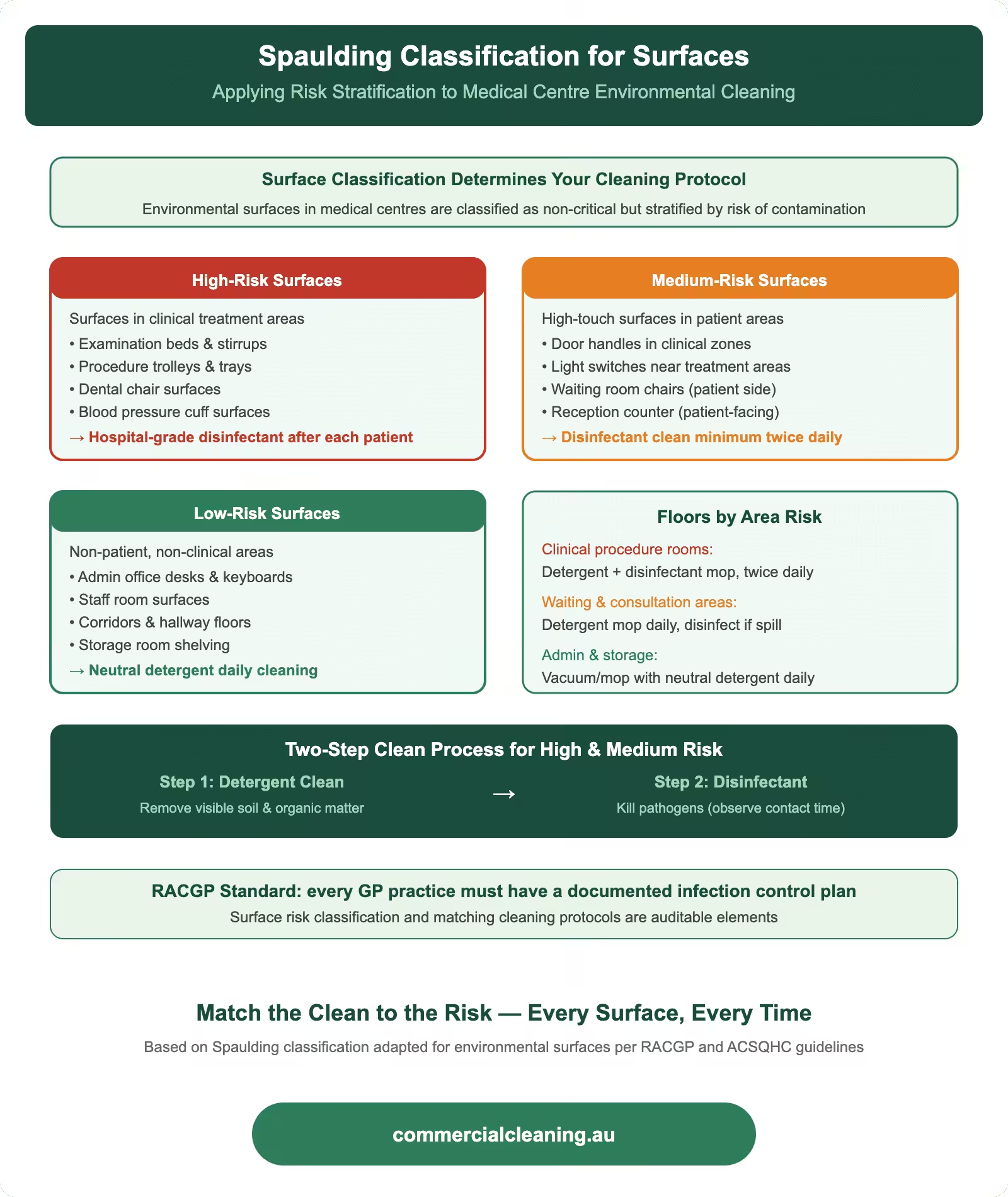
Spaulding classification applied to medical centre surfaces showing high, medium, and low risk categories with cleaning protocols and two-step process
Understanding the Spaulding Classification for Medical Centre Surfaces
Understanding the Spaulding Classification for Medical Centre Surfaces covers specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We always start our protocol development by mapping every surface in the facility against the Spaulding classification system, because this determines everything from chemical selection to contact time requirements. Our team has classified surfaces in over two hundred medical centres, and we find that most facilities underestimate how many semi-critical surfaces they actually have. We categorise each surface as critical, semi-critical, or non-critical, and we build our cleaning schedules around those classifications rather than applying a blanket approach.
Our work in Epping medical centres taught us that treatment room benchtops often function as semi-critical surfaces during minor procedures, even though many facilities treat them as non-critical. We have seen general practices where examination table surfaces were cleaned with the same low-level product used on waiting room chairs — a practice that fails to account for direct mucous membrane contact during skin assessments. We apply intermediate-level disinfection to every surface that could reasonably contact non-intact skin or mucous membranes, and we document our classification decisions so clinical staff can verify our rationale.
We have found that staff compliance improves dramatically when we provide colour-coded zone maps showing which Spaulding category applies in each room. Our teams in Marsfield and Eastwood medical centres use laminated reference charts mounted inside cleaning cupboards, giving our operatives instant visual confirmation of the correct chemical and method for every surface they encounter. We developed this system after noticing that verbal training alone resulted in roughly thirty percent classification errors during our internal audits.
Routine Cleaning Protocols by Medical Centre Zone
We divide every medical centre into functional zones because contamination risk varies enormously between a sterile procedure room and a general waiting area. Our protocols assign specific cleaning frequencies, chemical concentrations, and validation methods to each zone. We have refined this zoning approach across facilities in Epping, Eastwood, and Marsfield, and we consistently find that zone-based cleaning reduces cross-contamination incidents by margins our clients find remarkable. We treat each zone as its own micro-environment with distinct requirements.
Our clinical zone protocols require our teams to perform damp-dusting of all horizontal surfaces with hospital-grade disinfectant at the start of each session, followed by spot disinfection of high-touch points every sixty minutes during operating hours. We use microfibre cloths assigned by colour to specific zones — blue for clinical areas, green for general areas, red for bathrooms — and our operatives in Epping know that cross-zone cloth transfer is a termination-level offence. We have tracked our microfibre segregation compliance at ninety-eight percent across the past twelve months, which we attribute to rigorous induction training and unannounced spot checks.
Our waiting room and reception protocols focus on high-touch surface rotation. We clean door handles, reception counters, EFTPOS terminals, pen holders, and chair armrests on a two-hourly cycle during business hours. We introduced ATP bioluminescence testing at an Eastwood medical centre to validate our waiting room protocols, and we discovered that magazine surfaces carried higher bioburden than toilet flush buttons — a finding that convinced the practice to switch to digital entertainment displays. We now recommend this switch to every medical centre we service.
We pay particular attention to shared staff areas because these spaces often become overlooked contamination bridges between clinical and non-clinical zones. Our teams clean staff kitchen benchtops, fridge handles, microwave controls, and light switches with the same hospital-grade disinfectants we use in clinical areas. We made this decision after our Marsfield team identified Staphylococcus aureus on a staff room kettle handle during a routine ATP swab — a result that highlighted how staff movement between zones can transfer pathogens if intermediate spaces are cleaned to lower standards.
Healthcare Cleaning Risk Zone Comparison
Zone
Risk Level
Frequency
Disinfectant Grade
PPE Required
Operating Theatre
Critical
Between every case
Hospital-grade TGA
Full gown, gloves, mask
Patient Ward
High
2× daily + discharge
Hospital-grade TGA
Gloves, apron
Waiting Room
Medium
3× daily
Commercial-grade
Gloves
Admin Office
Low
Daily
General purpose
Gloves
Bathroom/Amenities
High
4× daily minimum
Hospital-grade TGA
Gloves, apron, eyewear
Terminal Cleaning Procedures Between Patients
Healthcare Cleaning Risk Zone Comparison requires specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We consider terminal cleaning the most critical element of any medical centre cleaning protocol because it represents the final barrier between one patient’s microbial load and the next patient’s exposure. Our terminal cleaning procedures go well beyond a quick wipe-down — we systematically address every surface within the treatment space using a defined sequence that prevents recontamination of already-cleaned areas. We always clean from the cleanest area to the most contaminated, working from high surfaces down to the floor, and from the far side of the room toward the door.
Terminal Cleaning Procedures Between Patients includes specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. Our teams follow a twelve-step terminal clean checklist that we developed after studying infection control audit data from over fifty medical centres we service across Sydney. We start with hand hygiene and PPE donning, then address light switches and door handles, followed by examination lights, equipment surfaces, benchtops, examination tables, stools, sinks, bins, and finally floors. We time our terminal cleans and maintain an average of fourteen minutes per standard consultation room — a figure we arrived at after determining that anything under ten minutes consistently produced unacceptable ATP readings on at least one surface.
We have invested in hydrogen peroxide vapour technology for deep terminal cleaning situations, particularly after confirmed cases of multi-drug-resistant organisms. Our Epping team deployed this technology three times in the past financial year, and post-treatment surface sampling returned zero colony-forming units on every tested surface. We believe this technology represents the gold standard for terminal disinfection in medical centres, though we recognise that its cost — approximately $2,690 per full-facility treatment — means most centres reserve it for outbreak situations rather than routine use.
Blood and Body Fluid Spill Management Protocol
We treat every blood and body fluid spill as a potential exposure event, and our protocols reflect the seriousness of that risk. Our teams carry dedicated spill kits in every medical centre we service, and we train our operatives to contain, treat, and remove spills in a specific sequence that minimises aerosolisation and splash risk. We have managed hundreds of spill incidents across our medical centre contracts, and our zero-exposure record for cleaning staff reflects the effectiveness of our approach.
Our small spill protocol — anything under ten centimetres in diameter — involves immediate application of granular absorbent, followed by careful collection into a clinical waste bag, then surface disinfection with sodium hypochlorite at ten thousand parts per million. We leave the disinfectant in contact for a minimum of ten minutes before final wipe and disposal. Our large spill protocol adds a perimeter containment step using absorbent pads, and we always don full PPE including face shield, fluid-resistant gown, and double gloves before approaching the spill zone. We developed these protocols in consultation with infection control practitioners at facilities across Epping and Eastwood.
We document every spill incident in our digital reporting system within fifteen minutes of resolution. Our reports capture spill type, estimated volume, location, time of discovery, response time, cleaning method, chemicals used, and final validation result. We have found that this documentation serves two purposes — it satisfies WHS record-keeping requirements and it provides data we use to identify spill hotspots. At one Marsfield practice, our spill data revealed that eighty percent of incidents occurred in one treatment room, which led to a workflow redesign that reduced spill frequency by half within three months.
Approved Disinfectants and Contact Times for Healthcare Settings
Approved Disinfectants and Contact Times for Healthcare Settings targets specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We select our disinfectant products based on three criteria: TGA registration, demonstrated efficacy against the specific pathogen risks present in each facility, and compatibility with the surface materials we encounter. Our product selection for medical centres differs significantly from our commercial cleaning range because healthcare environments demand hospital-grade formulations with proven kill claims against organisms like MRSA, VRE, and Clostridioides difficile. We review our chemical inventory quarterly and adjust our selections based on emerging resistance patterns reported by our infection control contacts.
Our standard disinfectant for non-critical surfaces in medical centres is a quaternary ammonium compound with a five-minute contact time, which we find balances efficacy with practical turnaround requirements. For semi-critical surfaces and terminal cleaning, we step up to accelerated hydrogen peroxide at the manufacturer’s recommended concentration, which gives us broad-spectrum efficacy including sporicidal activity at a ten-minute contact time. We have tested these products against the requirements of AS 4187.3 — the Australian standard governing cleaning and disinfection protocols for reusable medical devices — and we align our surface disinfection practices with the same evidence base that underpins instrument reprocessing standards.
We insist on strict contact time compliance because we have seen too many facilities where staff wipe surfaces with disinfectant and immediately dry them, effectively reducing the product’s efficacy to near zero. Our training emphasises that contact time is non-negotiable — the surface must remain visibly wet for the full specified duration. We use timer-based reminders on our team leader’s devices, and our Epping supervisor conducts weekly contact time audits using a stopwatch and observation checklist. Our compliance rate on contact time has reached ninety-four percent, up from sixty-one percent when we first introduced structured monitoring.
Clinical Waste Segregation and Disposal Compliance
We manage clinical waste segregation as an integrated component of our cleaning protocols because improper waste handling creates infection risks that can undo all the surface cleaning work we perform. Our teams segregate waste at the point of generation into clearly defined streams — general waste, clinical waste, cytotoxic waste, pharmaceutical waste, and sharps — using colour-coded containers that comply with AS/NZS 3816 requirements. We have found that the most common segregation error in medical centres is placing blood-contaminated items into general waste, which our training specifically addresses through scenario-based exercises.
Our waste management approach at Eastwood medical centres includes daily container audits where our team leaders inspect each waste stream for contamination. We photograph any misclassified items and report them to the practice manager with recommendations for staff re-education. We have reduced waste stream contamination rates across our medical centre contracts by forty-two percent since introducing photographic auditing eighteen months ago. We believe this visual feedback loop is far more effective than written incident reports because it gives clinical staff a concrete image of the error rather than an abstract description.
We coordinate with licensed clinical waste transporters to confirm chain-of-custody documentation meets EPA requirements from generation through to final treatment. Our digital tracking system records container weights, collection times, and transporter details for every pickup across our medical centre portfolio. We maintain these records for a minimum of five years, which exceeds the regulatory minimum and gives our clients complete audit trails should any compliance question arise.
Staff Training, PPE Requirements, and WHS Compliance
Staff Training, PPE Requirements, and WHS Compliance covers specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We invest more training hours per operative in our medical centre division than in any other part of our business because the consequences of error in healthcare environments are simply too significant. Every operative assigned to a medical centre contract completes our forty-hour healthcare cleaning induction, which covers infection control principles, Spaulding classification, chemical safety, spill management, waste segregation, and PPE donning and doffing sequences. We developed this programme in consultation with infection prevention nurses and WHS specialists, and we update the content annually based on new evidence and regulatory changes.
Our PPE requirements for medical centre cleaning exceed the minimums specified in most facility risk assessments because we believe in building safety margins. Our standard PPE for routine clinical area cleaning includes nitrile gloves, safety eyewear, closed-toe non-slip shoes, and a fluid-resistant apron. We step up to full barrier protection — including face shield, fluid-resistant gown, and double gloves — for terminal cleaning, spill management, and any task involving visibly contaminated surfaces. We conducted a PPE compliance audit across our Epping and Marsfield contracts last quarter and recorded ninety-seven percent compliance, with the three percent shortfall primarily involving eyewear omission during routine tasks.
We maintain competency records for every operative and require annual reassessment against our healthcare cleaning competency framework. Our framework covers twenty-three discrete competencies ranging from hand hygiene technique to chemical dilution accuracy. We use practical observation assessments rather than written tests because we have found that operatives who pass written exams sometimes struggle with real-world application. Our assessors observe each competency in a live cleaning situation and provide immediate corrective feedback where needed.
Environmental Cleaning Audit and Documentation
Environmental Cleaning Audit and Documentation involves specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. We audit every medical centre we clean on a monthly cycle using a structured assessment tool that covers all zones, all surface categories, and all procedural elements. Our audit framework draws on the National Safety and Quality Health Service Standards and incorporates ATP bioluminescence testing alongside visual inspection. We have found that visual inspection alone misses approximately twenty-five percent of surfaces that fail ATP testing, which is why we insist on objective measurement rather than relying solely on appearance. Our audit reports include zone-by-zone scores, trend analysis, and prioritised corrective actions.
Our documentation system captures every cleaning event, chemical batch number, dilution verification, and operative assignment in real time via tablet-based digital checklists. We transitioned from paper-based records three years ago, and the improvement in data completeness has been dramatic — our record completion rate jumped from seventy-two percent to ninety-nine percent within the first six months. We share monthly summary reports with each practice manager, and we provide full data access through a secure client portal. Our Epping clients have told us that this transparency gives them confidence they could not achieve with their previous cleaning provider.
We benchmark our audit results against national healthcare cleaning performance indicators and share comparative data with our clients so they can see how their facility performs relative to peers. Our current portfolio average sits at ninety-one percent compliance across all measured parameters, with our top-performing Marsfield facility consistently achieving ninety-six percent. We set a minimum threshold of eighty-five percent and trigger an immediate corrective action plan for any facility that falls below this benchmark in any audit cycle.
We encourage every practice manager to review our detailed findings alongside their own infection control data, because the correlation between cleaning audit scores and healthcare-associated infection rates is well established in the literature. Our team is always available to discuss results and collaborate on improvement strategies. For further guidance on treatment-specific disinfection procedures, we invite you to explore the next article in our medical cleaning series where we cover treatment room protocols in greater depth.
Frequently Asked Questions
Can we use the same disinfectant for all surfaces in the centre?
We would never recommend using a single disinfectant across all surfaces in a medical centre because different contamination levels and surface materials demand different chemical formulations. Our approach assigns quaternary ammonium compounds to non-critical surfaces where low-level disinfection is sufficient, accelerated hydrogen peroxide to semi-critical surfaces requiring intermediate-level disinfection, and sodium hypochlorite at elevated concentrations for high-risk spill situations. We select each product based on TGA registration status, surface compatibility, and demonstrated kill claims against the specific pathogens relevant to each zone. Using one product everywhere either over-treats low-risk areas — wasting money and potentially damaging sensitive surfaces — or under-treats high-risk areas, which creates genuine infection control gaps.
How often should we retrain staff on cleaning protocols?
We require all our medical centre operatives to complete formal refresher training at least annually, but our experience tells us that annual training alone is not enough to maintain consistent performance. We supplement annual sessions with monthly toolbox talks focused on specific topics like spill management or PPE compliance, and our team leaders conduct weekly observational coaching during routine shifts. We have found that this layered approach — combining formal training with ongoing reinforcement — keeps competency levels significantly higher than periodic classroom sessions alone. We also trigger immediate targeted retraining whenever our audits identify a specific skill gap in any operative.
What should we do if we identify a cleaning deficiency during an audit?
We treat every audit deficiency as a learning opportunity rather than a punitive event because our goal is sustained improvement rather than blame. Our corrective action process starts with identifying the root cause — whether it is a training gap, an equipment issue, a time pressure problem, or a procedural ambiguity. We then implement a targeted fix, assign responsibility for follow-up, and schedule a verification audit within fourteen days to confirm the correction has taken hold. We document every deficiency and its resolution in our continuous improvement register, and we review this register quarterly to identify systemic patterns that might indicate a need for broader protocol changes rather than individual corrections.
Are disinfectant wipes effective for all surfaces?
We use disinfectant wipes extensively for high-touch surfaces like door handles, light switches, and equipment controls because they deliver consistent chemical coverage and eliminate the risk of cross-contamination from shared cleaning solutions. However, we do not rely on wipes for large surface areas like examination tables or benchtops because a single wipe cannot deliver sufficient product to maintain the required contact time across a broad surface. For larger surfaces, we use spray-and-wipe methods with fresh microfibre cloths that allow us to apply adequate disinfectant volume and monitor contact time properly. We always check that our wipes carry the same TGA registration and kill claims as our liquid disinfectants.
How do we manage cleaning during a bloodborne pathogen exposure incident?
We activate our spill management protocol immediately upon notification of any bloodborne pathogen exposure. Our first priority is ensuring no unprotected person enters the affected area — we establish a visible exclusion zone using barrier tape or cones. Our operative then dons full barrier PPE before approaching the spill, applies granular absorbent to contain the material, and carefully collects all contaminated material into a clinical waste bag. We then apply sodium hypochlorite at ten thousand parts per million to the entire affected area and maintain contact for a minimum of ten minutes before final cleaning and disposal. We document the entire incident timeline and submit our report to the practice manager within one hour of resolution.
What AS standards apply to medical centre cleaning protocols?
We align our medical centre cleaning protocols with several Australian Standards, most notably AS 4187.3 which governs cleaning and disinfection practices for reusable medical devices and provides the evidence base for surface disinfection approaches in clinical settings. We also reference AS/NZS 3816 for clinical waste management, and we monitor updates to AS 5369 which covers healthcare facility cleaning more broadly. Our protocols incorporate guidance from the NHMRC Australian Guidelines for the Prevention and Control of Infection in Healthcare, which we consider the overarching framework within which all specific standards operate. We review standard updates quarterly to verify our procedures remain current.
How much does professional medical centre cleaning cost?
We find that medical centre cleaning costs vary considerably based on facility size, zone complexity, and service frequency. Our contracts for standard general practices with four to six consultation rooms typically start at around $1,800 per month for five-day-per-week service, while larger multi-specialty centres with procedure rooms and laboratory areas can range up to $4,500 monthly. We recently quoted a detailed protocol for a specialist centre in Epping that included terminal cleaning capability and hydrogen peroxide vapour access at $2,690 per month — a figure that reflected the facility’s higher-risk profile and our commitment to maintaining AS 4187.3 aligned procedures across every surface category.
Can your team handle cleaning during practice operating hours?
We design our medical centre cleaning schedules to work around practice operations because we understand that closing for cleaning is simply not practical for most facilities. Our standard approach delivers routine clinical zone cleaning during early morning hours before the first patient appointments, high-touch surface maintenance during the day between patient blocks, and terminal cleaning of treatment rooms between sessions or at end of day. We have refined this scheduling model across our Epping, Eastwood, and Marsfield contracts to make sure our presence never disrupts patient flow or clinical workflows while still maintaining the frequency our protocols demand.
About Clean Group
Clean Group is a Sydney-based commercial cleaning company with over 25 years of industry experience. Founded by Suji Siv, our team of 50+ trained professionals services offices, warehouses, medical centres, schools, childcare facilities, retail stores, gyms, and strata properties across Sydney, Melbourne, and Brisbane.
We are active members of ISSA and the Building Service Contractors Association of Australia (BSCAA). Our operations align with ISO 9001 (Quality Management), ISO 14001 (Environmental Management), and ISO 45001 (Workplace Health and Safety) standards. We hold membership with the Green Building Council of Australia and use eco-friendly, TGA-registered cleaning products wherever possible.
Every Clean Group cleaner is police-checked, fully insured, and trained in safe work procedures under SafeWork NSW guidelines. We operate 7 days a week, including after-hours and weekend services, to minimise disruption to your business.
Hi, I'm Suji Siv, the founder, CEO, and Managing Director of Clean Group, bringing over 25 years of leadership and management experience to the company. As the driving force behind Clean Group’s growth, I oversee strategic planning, resource allocation, and operational excellence across all departments. I am deeply involved in team development and performance optimization through regular reviews and hands-on leadership.