Medical Pathology Lab Disinfection Protocols: Contamination Control for Australian Laboratories

Pathology laboratories in Sydney operate under strict regulatory frameworks that demand precision in every aspect of facility management. When you’re running a PC2 or PC3 laboratory in suburbs like Westmead, Randwick, or Macquarie Park, contamination control isn’t a convenience—it’s a legal obligation and a direct reflection of your diagnostic accuracy. Our team has cleaned hundreds of pathology labs across greater Sydney, and we’ve learned that the difference between compliant facilities and those facing regulatory action comes down to one thing: understanding what your auditors are actually looking for. This guide covers the decontamination, cleaning, and disinfection protocols that NATA accreditation bodies examine, the specific chemical and physical systems that work in Australian laboratories, and the practical steps your team needs to implement medical cleaning standards that stick.
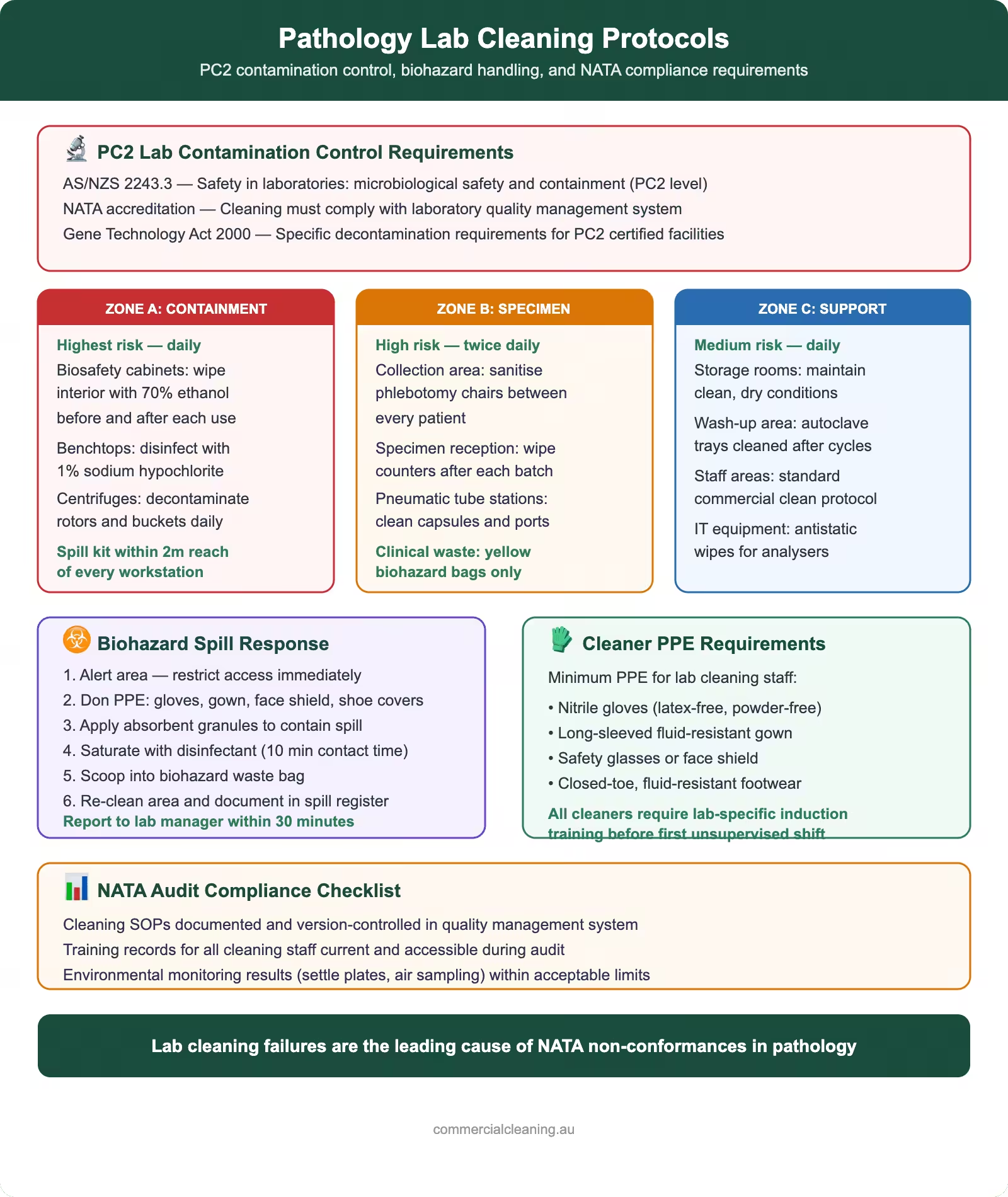
Contamination Control Requirements for PC2 Pathology Labs
Contamination Control Requirements for PC2 Pathology Labs covers specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. Physical Containment Level 2 is the most common classification for Australian pathology laboratories. Under AS/NZS 2243.3 (Safety of the Laboratory Environment — Microbiological Safety), PC2 facilities must handle organisms that pose a moderate hazard to humans but won’t spread between patients without close contact.
We worked with a major laboratory network across St Leonards and Kogarah last year, and their NATA auditor explicitly checked for three things: surface integrity (are benchtops cracked, allowing bacterial seepage?), air handling system documentation (is negative pressure maintained?), and decontamination logs (do staff actually record what they cleaned and when?). Many labs pass the first two because the infrastructure is in place. They fail on the third because cleaning teams don’t understand what’s being audited.
PC2 requirements under WHS Regulation 2017 demand that:
- Work surfaces are impervious and can be decontaminated without damage
- Staff access biosafety cabinets (Class I or Class II Type A2 minimum)
- Laboratory design prevents aerosol escape during centrifugation, incubation, and sample processing
- Chemical and biological spill containment is immediate and documented
- All staff complete competency training in hazard recognition and decontamination procedures
Mycobacterium tuberculosis, MRSA, Hepatitis B, and Cryptosporidium are pathogens regularly present in PC2 facilities. Your cleaning protocols must account for their survival on surfaces—some bacteria persist for weeks on dry surfaces—and their resistance to common disinfectants. Sodium hypochlorite at 1000 ppm is the baseline for most organic contamination, but tubercle bacilli require contact times of at least 10 minutes. Your disinfectant selection isn’t optional; it’s dictated by the specific pathogens your laboratory confirms.
Three-Stage Lab Cleaning Protocol: Decontaminate, Clean, Disinfect
Three-Stage Lab Cleaning Protocol involves specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. This sequence isn’t arbitrary. Each stage serves a specific function, and skipping or reversing steps renders the entire cleaning process ineffective.
Stage 1: Decontamination involves neutralising biological or chemical hazards before cleaning begins. If a vial of Hepatitis C specimen breaks, you don’t immediately wipe it with a cloth. You first contain the spill, apply absorbent granules if required, spray with a disinfectant like Virkon S or Viraclean (Whiteley Medical), and allow full contact time—typically 10 to 30 minutes depending on the product. Only after contact time has passed do you remove contaminated material and place it in a yellow clinical waste bin compliant with AS/NZS 3816.
Our team at a Westmead laboratory learned this the hard way when a technician cleaned a blood spill immediately after spraying disinfectant, reducing contact time from 30 minutes to 2 minutes. The environmental monitoring settle plates taken the next day showed viable pathogens still present. NATA later flagged the incident during accreditation review.
Stage 2: Cleaning removes organic soil, dust, and residues using detergent and mechanical action. This is where most labs think the work is done, but in fact, disinfectants don’t work effectively on dirty surfaces. Mycobacteria and norovirus hide in biofilm and organic matter. You must clean first—using hot water, neutral pH detergent, and a cloth or brush to physically remove buildup—before any disinfectant can make contact with microbial cells.
Stage 3: Disinfection uses validated chemical agents to kill remaining microorganisms. The product choice depends on your pathogen profile, surface material, and contact time constraints. For general PC2 work across epoxy resin or stainless steel benchtops, 70% isopropyl alcohol is sufficient for low-contamination areas, but high-risk surfaces (centrifuge rotor chambers, biosafety cabinet work surfaces) require broader-spectrum agents like 10,000 ppm sodium hypochlorite or Trigene (Medichem) when chlorine-based disinfectants would corrode equipment.
| Contamination Level | Disinfectant Product | Contact Time | Surface Material |
|---|---|---|---|
| Low (no blood/tissue) | 70% Isopropyl alcohol | 1 minute | Stainless steel, epoxy resin |
| Moderate (blood/bodily fluids) | Sodium hypochlorite 1000 ppm | 10 minutes (TB) / 5 minutes (other) | Epoxy resin, vinyl flooring |
| High (TB, fungi, viruses) | Sodium hypochlorite 10,000 ppm or Viraclean | 30 minutes | Epoxy resin, vinyl flooring (not stainless steel) |
| Instrument/equipment safe | Trigene or Virkon S | 15 minutes | All surfaces, including stainless steel |
Contact time is enforced by a simple rule: don’t let the surface dry before the contact time window closes. If you spray a bench with 1000 ppm sodium hypochlorite at 9:00 AM and it dries by 9:05 AM, you’ve lost the disinfection benefit. Your cleaning team must either spray and re-wet at intervals or cover the surface to prevent evaporation. Auditors ask to see photos or video evidence of this practice.
Biosafety Cabinet Decontamination Procedures
Biosafety cabinets are the literal and figurative centrepiece of PC2 laboratory contamination control. They are the barrier between your staff and the organisms they’re handling. In our experience cleaning Class II Type A2 cabinets across Campbelltown and Liverpool laboratories, we’ve seen that most facilities follow the manufacturer’s quarterly decontamination schedule but skip the critical between-use wiping protocol.
Class II Type A2 cabinets in use must be wiped down at the end of every working day with 70% isopropyl alcohol. This removes loose microbial particles before they settle into crevices or bypass the HEPA H14 exhaust filter. Weekly, the interior work surface should be cleaned with detergent, then disinfected with 1000 ppm sodium hypochlorite or an equivalent product. Quarterly or after known contamination events, full fumigation may be required.
Fumigation protocols vary by cabinet model, but the legacy formaldehyde method (using formalin gas) is less common in Australia now. Most manufacturers recommend hydrogen peroxide vapour (HPV) systems or peracetic acid fogging because they leave no toxic residues and are less labour-intensive. These require the cabinet to be sealed, the decontaminant introduced under controlled conditions, and a contact time of 12–24 hours depending on the method. After fumigation, the cabinet must be purged and HEPA filter integrity tested using a DOP (dioctyl phthalate) or PAO (polyalphaolefin) aerosol challenge to confirm the filter wasn’t compromised and still removes 99.995% of particles ≥0.5 μm.
We consulted with a laboratory in Macquarie Park where staff assumed quarterly professional fumigation was sufficient. When NATA conducted an audit, they requested evidence of the DOP test results. The laboratory had no documentation. NATA required them to engage a certified firm (carrying accreditation from Standards Australia) to conduct the test and certify the cabinet’s performance. This cost them $600 per cabinet and a corrective action notice. Documentation matters as much as the physical cleaning.
Biosafety cabinet cleaning checklist:
- Daily: wipe work surface with 70% isopropyl alcohol; inspect for spills or debris
- Weekly: deep clean interior surfaces and edges using detergent and brush; apply 1000 ppm sodium hypochlorite or equivalent; contact time minimum 5 minutes
- Monthly: check sash function, light bulbs, and UV-C bulb (if present) for degradation
- Quarterly or post-contamination: arrange professional HPV or peracetic acid fumigation; confirm DOP/PAO filter integrity testing within 72 hours
- Annual: arrange professional HEPA filter inspection and airtightness certification
Chemical Spill Management and Emergency Decontamination
Chemical Spill Management and Emergency Decontamination includes specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. Spills in pathology laboratories are not unusual—they’re routine events. The difference between a controlled incident and a regulatory failure is your written protocol and your team’s training.
Under AS/NZS 2243.3 and the WHS Act 2011, every facility must maintain a spill kit readily accessible to laboratory areas. The kit should contain absorbent granules (not sawdust, which can float), neutralising agents (sodium bicarbonate for acids, dilute acid for bases), forceps or tongs, disposable gloves, and a sharps container. Staff must know the location of every spill kit and understand that spill management is not the cleaning team’s exclusive responsibility—it begins with the laboratory technician who caused the spill.
Our team responds to emergency decontamination calls in Sydney, and we’ve found the most dangerous scenarios happen when laboratory staff attempt to clean up hazardous spills themselves without contacting cleaning specialists. A research scientist in Randwick applied isopropyl alcohol to a cytotoxic drug spill without proper containment; the fumes affected multiple staff members. Cytotoxic agents like docetaxel and paclitaxel require specific neutralisation steps and are regulated under TGA guidelines. They cannot be treated like standard biological spills.
Emergency decontamination sequence:
- Evacuate the immediate area. If airborne exposure is suspected, activate building ventilation and move personnel upwind.
- Contain the spill using absorbent granules or spill mats (pre-positioned near biosafety cabinets). Prevent spreading by using barriers or tape.
- Contact your external cleaning team and SafeWork NSW if the spill involves a reportable quantity of hazardous substance (defined under NSW EPA guidance).
- Disinfect with appropriate agent: 1000 ppm sodium hypochlorite for blood/bodily fluids; 10,000 ppm for TB/fungal contamination; specific neutralisers for chemical hazards (consult SDS).
- Dispose of contaminated material in appropriate clinical waste container (yellow for infectious, red for cytotoxic, purple for cytotoxic sharps).
- Document the incident in a formal spill log with date, time, location, nature of spill, remedial action, staff involved, and notification contacts.
Chemical resistance of your spill kit materials is critical. Paper towels won’t work with volatile organics; you need lint-free wipes or absorbent granules. Plastic containers will degrade if exposed to certain solvents. Your spill kit should be inspected and refreshed every six months, and your team should run tabletop drills annually to confirm staff know the protocol without hesitation.
Laboratory Surface Materials and Chemical Resistance
Laboratory Surface Materials and Chemical Resistance addresses specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. You cannot clean surfaces you don’t understand. A benchtop that looks uniform to the naked eye may combine three different materials, each with different cleaning and disinfection tolerances.
Epoxy resin is the gold standard in Australian pathology laboratories because it’s chemical resistant, washable, and allows disinfectants to make full contact. In our experience, epoxy benchtops in Westmead facilities withstand 1000 ppm sodium hypochlorite, 70% isopropyl alcohol, and even 10,000 ppm hypochlorite without degradation if contact time is controlled and the surface is rinsed thoroughly afterward. However, prolonged exposure to high-concentration hypochlorite (several hours) can cause dulling and micro-etching. Your cleaning schedule should assume contact times of 10–30 minutes, not overnight soaking.
Phenolic resin is common in older laboratories and is more fragile than epoxy. It resists standard disinfectants but can absorb liquid if scratched or aged. If you’re cleaning a phenolic resin surface, avoid abrasive cloths and extended contact with high-concentration solutions. 70% isopropyl alcohol and low-concentration sodium hypochlorite (1000 ppm, 5-minute contact) are safer choices.
Stainless steel (316 grade, preferred for corrosion resistance) is used for sink areas, instrument racks, and autoclave chambers. Sodium hypochlorite corrodes stainless steel, especially above 1000 ppm and beyond 5 minutes contact time. If you must disinfect stainless steel, use Trigene, Virkon S, or 70% isopropyl alcohol. Always rinse thoroughly with water afterward and dry to prevent chloride residue from settling into surface irregularities.
Chemical-resistant vinyl flooring with coved edges (where the floor meets the wall in a smooth curve, preventing dirt accumulation in corners) is standard in PC2 labs. Vinyl tolerates most disinfectants but can become slippery if oversaturated. Spray and wipe rather than flood-clean. Check the floor regularly for tears or peeling at seams; if the substrate is exposed, bacteria will colonise the gap and your flooring is compromised until repair.
Material compatibility matrix for common lab surfaces:
| Surface Material | Safe Disinfectants | Avoid | Inspection Notes |
|---|---|---|---|
| Epoxy resin benchtops | Sodium hypochlorite (all concentrations), 70% IPA, Viraclean, Trigene | None (all are compatible) | Check for cracks or voids; deep clean seams quarterly |
| Phenolic resin benchtops | 70% IPA, sodium hypochlorite ≤1000 ppm (5-min contact) | High-concentration bleach, abrasive scrubbing | Inspect for discolouration or swelling; replace if damaged |
| Stainless steel (316 grade) | 70% IPA, Trigene, Virkon S | Sodium hypochlorite >1000 ppm, prolonged high-concentration exposure | Dry thoroughly after cleaning to prevent chloride pitting |
| Chemical-resistant vinyl flooring | All disinfectants (spray and wipe method) | Flood-cleaning, abrasive equipment | Inspect seams for separation; check for tears or punctures |
| Plastic/polycarbonate equipment | 70% IPA, mild detergent solutions | Sodium hypochlorite, Viraclean, harsh solvents | Wipe dry immediately; heat and chemicals can cause warping |
When we conduct a laboratory cleaning audit, one of the first things we assess is whether the cleaning team knows the benchtop material. We’ve found that many facilities stock only one or two disinfectants and assume they work everywhere. This assumption fails when you encounter a mix of epoxy and phenolic, or when stainless steel instrument racks get sprayed with high-concentration bleach. Your written cleaning protocol must specify the disinfectant for each zone of the laboratory.
Clinical Waste Segregation Under AS/NZS 3816
Clinical Waste Segregation Under AS/NZS 3816 targets specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. Contaminated materials don’t become non-hazardous because you’ve sprayed disinfectant on them. They remain hazardous waste until they’re segregated, treated, and disposed of according to AS/NZS 3816 (Medical Waste Management).
Australian pathology laboratories produce three main types of clinical waste:
- Yellow bins: Infectious or potentially infectious waste—blood, bodily fluids, cultures, contaminated sharps, specimen containers, swabs, and tissue samples. This category includes almost everything that contacts patient samples in a pathology lab.
- Red bins: Chemotherapy and other cytotoxic waste—materials contaminated with docetaxel, paclitaxel, bleomycin, and similar agents. These are more hazardous than general infectious waste and require specialised incineration facilities.
- Purple bins: Cytotoxic sharps—needles, pipette tips, and glass contaminated with chemotherapy agents. These require both sharps handling safety (AS 4031) and cytotoxic waste protocols.
We worked with a Liverpool laboratory that mixed cytotoxic waste into yellow bins; the waste contractor noticed during segregation and imposed a surcharge plus a corrective action notice from NSW EPA. The laboratory also faced an NATA audit finding because waste segregation failure indicates inadequate staff training in hazard recognition.
Your cleaning team is not responsible for generating waste, but you are responsible for understanding what gets placed in each bin and for identifying segregation errors. If you encounter mixed waste (a micropipette tip in a yellow bin, or yellow waste in a red bin), flag it immediately and don’t move it. Document the incident and use it as a training opportunity. Waste handlers depend on accurate segregation; incorrect bins can expose them to unexpected hazards.
Sharps containers must comply with AS 4031 and be puncture-proof, colour-coded (yellow for standard sharps, purple for cytotoxic sharps), and sealed before removal from the laboratory. They should not be overfilled; once they reach the fill line, they must be replaced. We’ve observed sharps containers left open or stored in hallways—both are violations that auditors flag immediately.
NATA Accreditation: What Auditors Check in Your Cleaning Program
NATA accreditation for pathology laboratories is rigorous, and cleaning is a core audit element. Auditors don’t just inspect surfaces; they review your documentation systems, staff training records, chemical inventory, and environmental monitoring data.
When a NATA auditor arrives at a facility in Macquarie Park or St Leonards, they will:
- Review cleaning logs — Do staff record what was cleaned, when, with which product, and for how long? Are contact times documented? Is there evidence of supervisor sign-off?
- Inspect surfaces under UV light — Does epoxy resin fluoresce, indicating residual biological material? Are benchtop seams clean?
- Test surfaces with ATP bioluminescence — ATP testing shows adenosine triphosphate (a marker of cellular contamination). If results exceed baseline thresholds, the surface wasn’t adequately cleaned. We use ATP testing on every job; if a benchtop reads >100 RLU (Relative Light Units), we re-clean immediately.
- Request certifications — Fumigation reports, DOP/PAO filter test certificates, waste handler permits, chemical SDS sheets, and staff training records must be produced on demand. If you don’t have a document, assume the auditor will ask for it.
- Interview staff — Do cleaning personnel understand which disinfectant to use on stainless steel vs. epoxy? Can they describe the three-stage protocol? Can they identify a spill kit and explain emergency response?
- Conduct environmental monitoring — Auditors may commission settle plates (petri dishes left open for 4 hours to capture airborne and settling particles) or swab high-touch surfaces for viable pathogen recovery. Results feed back into your corrective action plan.
Our team has supported laboratories through NATA audits, and the most common deficiency we see is incomplete documentation. A laboratory will have excellent cleaning practices but no written protocol or no dated records. NATA operates on the principle that if it’s not documented, it didn’t happen. Even if your facilities are spotless, you’ll receive a corrective action if you can’t produce a cleaning log for the past 12 months.
Common NATA findings related to cleaning:
- Cleaning procedures not validated against specific pathogens handled by the laboratory
- Staff training in hazard recognition and decontamination not current or documented
- Spill response protocols not written or staff unfamiliar with procedures
- Disinfectant contact times not enforced (surfaces dried too quickly)
- Biosafety cabinet fumigation and DOP test certificates missing or outdated
- Waste segregation errors indicating inadequate staff awareness
- Environmental monitoring data not reviewed or acted upon
The solution is a three-part system: written procedures, trained personnel, and ongoing documentation. We provide laboratories with cleaning protocol templates that align with AS/NZS 2243.3, WHS Regulation 2017, and NATA expectations. We train staff annually. And we maintain a digital cleaning log that supervisors sign off on daily. When NATA arrives, all documentation is ready.
Staff Training and Competency for Lab Cleaning
Staff Training and Competency for Lab Cleaning covers specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. A well-designed laboratory with perfect equipment is only as effective as the people using it. Under WHS Regulation 2017 and NATA accreditation standards, laboratory staff must demonstrate competency in hazard recognition, decontamination procedures, and emergency response.
Initial training should cover:
- Biological hazards relevant to your facility (PC level, specific pathogens, routes of exposure)
- Chemical disinfectants: how they work, contact times, safety data, incompatibilities with surfaces and other substances
- The three-stage protocol: decontamination, cleaning, disinfection with worked examples
- Biosafety cabinet operation and between-use care procedures
- Spill response: containment, notification, decontamination, documentation
- Waste segregation under AS/NZS 3816: which bin for which material, why segregation matters
- Personal protective equipment (PPE): when gloves are required, when respiratory protection is needed, proper donning and doffing
- Environmental monitoring: why we use settle plates or ATP testing, how to interpret results
We conducted staff training across a Kogarah laboratory network, and the feedback was consistent: staff knew cleaning was important but didn’t understand the science behind contact time or why phenolic and epoxy benchtops needed different products. Once we explained that disinfectants kill microbes by denaturing proteins or disrupting cell membranes—and that this takes time—staff became more diligent about respecting contact times. They stopped rushing and started documenting. Competency improves when people understand the why, not just the what.
Refresher training should occur annually and immediately after any incident (spill, contamination, regulatory finding). If NATA identifies a cleaning deficiency, retraining of the affected area is mandatory. Your laboratory should maintain a training register with attendee names, dates, topics, and trainer credentials. SafeWork NSW expects this documentation if an incident occurs.
Competency assessment is not a one-time checklist. Observable competency includes:
- Correctly identifying disinfectant products and explaining their uses
- Demonstrating proper spray-and-contact technique without shortcuts
- Troubleshooting contamination (e.g., if a settle plate shows high microbial counts, staff can suggest likely causes and corrective actions)
- Responding to spills calmly and following the written protocol
- Communicating hazards and cleaning status to laboratory supervisors
Your cleaning team should feel empowered to ask questions and raise concerns. If a staff member notices a crack in a benchtop or suspects inadequate disinfection, they should be able to flag it without fear. A healthy laboratory culture treats cleaning as skilled work, not a routine chore.
Frequently Asked Questions
How often should biosafety cabinets be professionally fumigated?
Biosafety cabinet fumigation depends on usage intensity and contamination events. The manufacturer’s maintenance schedule typically specifies quarterly (every 3 months) for heavy-use cabinets in PC2 or PC3 labs. However, if your laboratory handles pathogens with high spill risk or if environmental monitoring reveals viable organism recovery in or near the cabinet, fumigation may be needed monthly. After any known contamination event—a culture spill, broken vial, or visible aerosol release—fumigation should be arranged within 48 hours. We recommend maintaining a schedule and sticking to it rather than delaying until a problem appears.
What disinfectant should we use on laboratory floors?
Laboratory floors in pathology facilities are typically vinyl with coved edges, and they tolerate most disinfectants. For routine daily cleaning of low-contamination areas, 70% isopropyl alcohol is adequate. For areas where blood or bodily fluids may have contacted the floor (near collection benches, waste disposal areas), 1000 ppm sodium hypochlorite is appropriate, sprayed and wiped—not flooded. High-traffic areas should be cleaned at least daily; if environmental monitoring shows microbial counts above baseline, increase frequency to twice daily or switch to a broader-spectrum disinfectant like Viraclean or Virkon S. Always check with your floor manufacturer to confirm compatibility with your chosen disinfectant.
How do I know if my cleaning protocol is adequate?
Environmental monitoring is your answer. Settle plates (petri dishes left open in the work area for 4 hours) capture airborne particles and settling microbes. After cleaning, colony counts should be zero or very low (typically <1 per plate in clean labs). If your settle plates consistently show ≥5 colonies, your cleaning protocol needs adjustment: increase contact time, switch to a broader-spectrum disinfectant, or increase cleaning frequency. ATP bioluminescence testing of cleaned surfaces provides rapid feedback—if a benchtop reads >100 RLU after cleaning, it’s not clean enough. NATA auditors expect to see environmental monitoring data reviewed and acted upon, so establish a baseline and track trends over time.
Are bleach-based disinfectants always the best choice for pathology labs?
Sodium hypochlorite (bleach) is effective and inexpensive, making it popular in many laboratories. However, it has limitations: it corrodes stainless steel at high concentrations, has a strong odour, can damage some plastic equipment, and breaks down quickly once diluted. For these reasons, non-chlorine alternatives like Trigene, Virkon S, or Viraclean may be preferable for sensitive equipment or areas with stainless steel surfaces. Each facility should evaluate their pathogen profile, surface materials, and staff tolerance for odour before selecting a primary disinfectant. Most laboratories use a combination—sodium hypochlorite for general bench work, 70% isopropyl alcohol for low-contamination areas and stainless steel, and a non-chlorine agent like Trigene for equipment-heavy zones.
What should I do if I find mixed waste in a clinical waste bin?
Do not touch it. Document what you observe (take a photo if possible), note the date, time, and location, and immediately notify your laboratory supervisor and waste management team. Mixed waste indicates a breakdown in staff training or procedural compliance. It must be segregated correctly before removal to prevent exposing waste handlers to unexpected hazards. Your laboratory should use this as a trigger for immediate retraining and a review of your waste segregation protocol. Repeated segregation errors will be flagged as corrective actions in NATA audits and NSW EPA inspections.
About Clean Group
Clean Group is a leading commercial cleaning company in Sydney, providing professional cleaning services to offices, strata buildings, medical facilities, schools, gyms, and retail spaces across the greater Sydney region. With over 25 years of experience and a commitment to WHS compliance, eco-friendly practices, and consistent quality, Clean Group delivers tailored cleaning solutions backed by a 100% satisfaction guarantee.
If your pathology laboratory requires specialist decontamination, biosafety cabinet cleaning, or staff training in compliance with AS/NZS 2243.3, AS/NZS 3816, and NATA accreditation standards, our team is ready to support your facility. We work across Westmead, Randwick, St Leonards, Macquarie Park, Liverpool, Campbelltown, and Kogarah. Contact us for a consultation and cleaning audit tailored to your laboratory’s specific needs. We also offer clinic cleaning protocols for allied health facilities including physiotherapy and podiatry clinics, extending the same rigorous contamination control practices across healthcare settings. For comprehensive cleaning protocols specific to other healthcare environments, see our guide on biohazard spill response.
About the Author
Suji Siv
/

Hi, I'm Suji Siv, the founder, CEO, and Managing Director of Clean Group, bringing over 25 years of leadership and management experience to the company. As the driving force behind Clean Group’s growth, I oversee strategic planning, resource allocation, and operational excellence across all departments. I am deeply involved in team development and performance optimization through regular reviews and hands-on leadership.
Read More About Suji