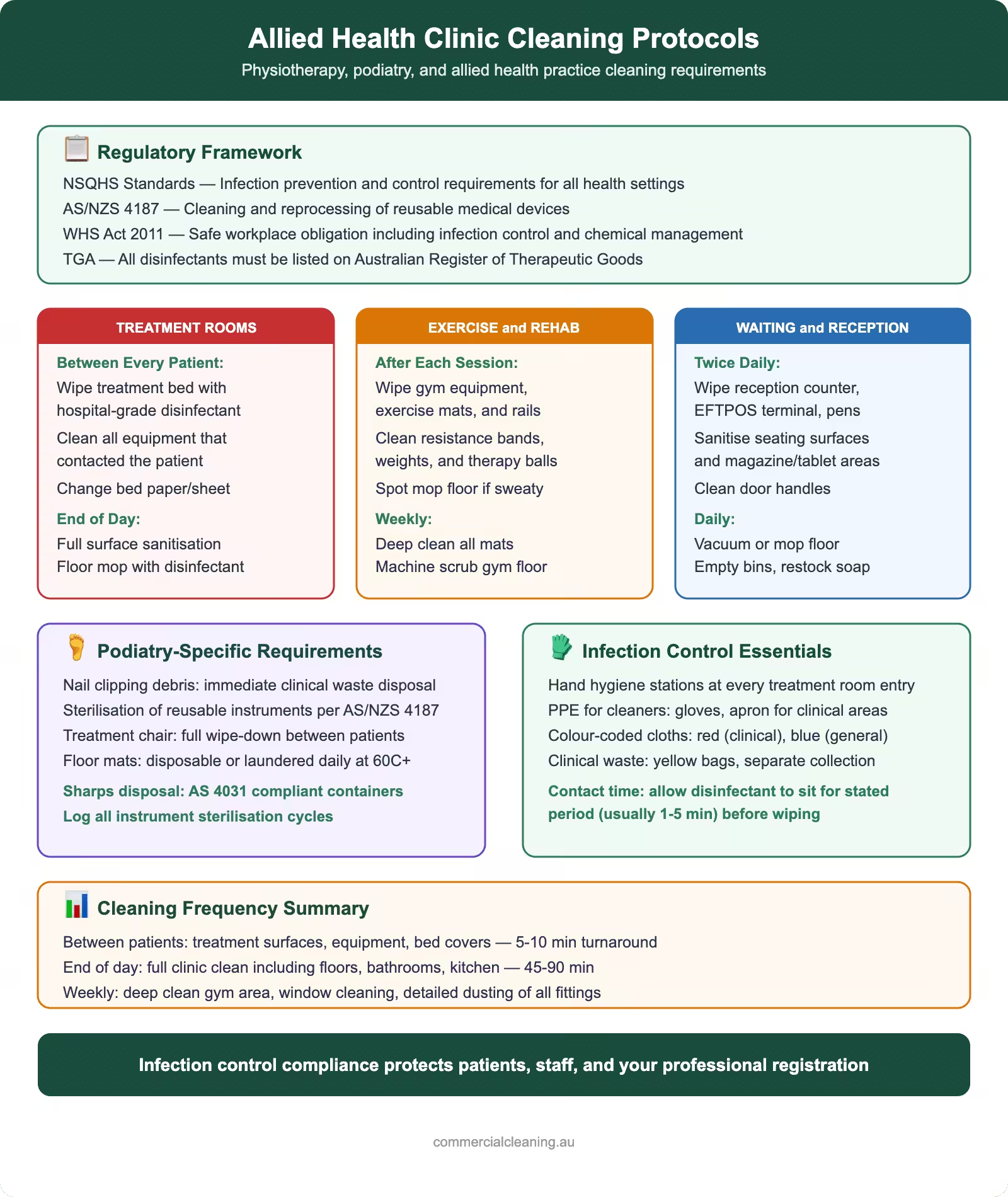
Allied health clinic cleaning protocols showing regulatory framework, treatment room and exercise area cleaning standards, podiatry requirements, and infection control essentials
Regulatory Framework for Allied Health Clinic Cleaning in Australia
Allied health clinics—physiotherapy practices, podiatry surgeries, and multidisciplinary treatment centres—require careful medical cleaning to meet strict infection control and workplace safety requirements across NSW and Australia. The primary governing framework comes from the Work Health and Safety Act 2011 and WHS Regulation 2017, which require clinic managers to manage biological hazards and maintain safe premises. Healthcare facility cleaning standards are integral to this compliance. Beyond WHS, your clinic must comply with the Physiotherapy Board of Australia and Podiatry Board of Australia practice standards, which explicitly reference environmental cleanliness as a patient safety measure.
We’ve found that many clinics miss the National Safety and Quality Health Service (NSQHS) Standards connection, even though private allied health clinics seeking accreditation must align with these standards. AHPRA (the Australian Health Practitioner Regulation Agency) doesn’t directly audit cleaning, but it will review breach notifications if poor hygiene leads to patient harm. The TGA (Therapeutic Goods Administration) regulates sterilisation equipment and disinfectant products your clinic uses, so any claims about antimicrobial effectiveness must be backed by TGA ARTG registration.
SafeWork NSW publishes guidance specific to healthcare settings, and for clinics in the Greater Sydney area—Chatswood, Parramatta, Bondi Junction, Hurstville, Penrith, Bankstown, and Hornsby included—this is your enforcement body. They inspect based on risk, and documented cleaning schedules and infection control policies demonstrate due diligence. Our team at a Parramatta physio clinic last year was asked by a SafeWork inspector for evidence of post-contact disinfection protocols; having detailed records made compliance assessment simple.
Environmental Risk Assessment: Classifying Your Clinic Spaces
Environmental Risk Assessment involves specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. Not all areas of your clinic pose the same infection risk. The Spaulding classification system—developed for surgical instruments but applied to all clinical environments—helps you stratify your cleaning effort correctly. Understanding where your true risk lies prevents over-cleaning some areas while under-protecting others.
In a physio clinic, your reception/waiting area is low-risk (non-critical). Patients are seated, no blood exposure occurs, and standard commercial cleaning (daily damp dusting, sanitising high-touch surfaces) is appropriate. Your treatment rooms with tables and equipment are semi-critical: the vinyl or PU leather-upholstered treatment tables can contact minor skin abrasions or non-intact skin, ultrasound transducer heads touch intact skin but can transmit pathogens if not cleaned between patients, and exercise equipment may be touched by multiple people. These require between-patient disinfection with a TGA-registered intermediate-level disinfectant.
Podiatry clinics increase risk significantly. Procedure rooms where you perform nail debridement, removal of warts, or skin lesion work are semi-critical (and occasionally critical if sharp instruments break skin). The podiatry chair, foot bath, nail drill stations, and scalpel handles all require higher-level disinfection protocols. If your podiatry practice includes minor surgical procedures (removal of ingrown toenails under local anaesthesia), those spaces and instruments move into the critical category and demand steam sterilisation.
The instrument sterilisation/storage room is where you manage reusable medical devices. This area requires environmental control (low dust, low humidity, temperature stability) and careful workflow separation (clean side vs. contaminated side). An environmental risk assessment matrix—which SafeWork NSW encourages you to document—lists each functional area, the pathogens present (Staphylococcus aureus, MRSA, Pseudomonas aeruginosa, fungal organisms like Trichophyton for tinea pedis, and HPV for plantar warts), and the required cleaning frequency and agent. Our experience cleaning allied health clinics in Hornsby and Bondi Junction shows that clinics without this formal matrix often miss hand basin areas and orthopaedic bracing storage zones.
Enzymatic cleaners during processing; detergent only for environmental surfaces
Bathrooms / amenities
Non-critical
Daily + 2–3 times per day if high-patient volume
General bathroom disinfectant or detergent + bleach solution
Daily, Weekly and Monthly Cleaning Schedules for Physio and Podiatry Clinics
Daily, Weekly and Monthly Cleaning Schedules for Physio and Podiatry Clinics requires specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. A structured schedule prevents missed areas and demonstrates compliance to AHPRA, SafeWork NSW, and auditors from the Clinical Excellence Commission (NSW). Our team at clinics across Chatswood, Parramatta, and Bankstown uses a tiered approach: immediate (between-patient), daily terminal, weekly, and monthly deep cleans.
Between-patient cleaning (immediate): After each patient departs, treatment tables, electrode pads (if TENS/EMS used), ultrasound transducers, and any equipment the patient touched must be wiped with a single-use cloth or disposable wipe dampened with intermediate-level disinfectant. For physio: a 1:10 dilution of Viraclean, applied, left for 30 seconds contact time, then wiped dry. For podiatry: the same for nail drill handles, scalpel handles, curettes, and the podiatry chair seat and footrest. Foot baths require draining and a wipe-down with enzymatic pre-cleaner followed by intermediate disinfectant. Hand basins should be cleaned, and staff should perform alcohol-based hand rub (ABHR) or hand washing. This process takes 2–3 minutes per patient and is non-negotiable under AS 5369:2023.
Hand-touch sites—door handles, light switches, reception desk, appointment book/computer mouse—require disinfection 2–3 times daily in higher-traffic clinics. We’ve found that using colour-coded cloths (red for high-touch, blue for equipment) helps staff track what’s been done.
Daily terminal clean (end of shift): After the last patient, a thorough clean of all treatment rooms, waiting areas, and bathrooms. This includes vacuuming carpeted areas (or dry mopping if hard floors), damp mopping with detergent and water, then spot-disinfecting all patient-contact surfaces. In a podiatry clinic, this also means cleaning out and disinfecting foot bath lines, emptying bins, and removing any visible soil from floor drains. Staff bathrooms and hand basins receive a detergent and disinfectant clean.
Weekly deep clean: Scheduled once weekly (typically after-hours or early morning), this includes damp-dusting high shelves, cleaning inside equipment (ultrasound gel bottles, foot bath controls), sanitising door frames, disinfecting waiting room seating, and inspecting floor grout for staining. In our experience cleaning a Hurstville physio clinic, we found that weekly attention to under-table crevices where lint accumulates prevents a build-up that can harbour dust mites and skin cells.
Monthly and quarterly deep cleans: Equipment like hot packs, cold packs, exercise balls, and resistance bands are wiped down and air-dried. Air conditioning vents are vacuumed. If your clinic uses an autoclave or instrument washer, the exterior and accessible interior surfaces are cleaned. Orthotic grinding stations (if podiatry) receive extraction filter changes and a thorough dust-down. Wall-mounted shelving in the sterilisation room is wiped with detergent.
TGA-Approved Disinfectants: Product Selection for Allied Health
TGA-Approved Disinfectants includes specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. Choosing the right disinfectant for allied health practice is a technical decision, not a price one. The TGA maintains the Australian Register of Therapeutic Goods (ARTG), which lists all registered disinfectant products with claims for specific pathogens and contact times. Selecting a TGA ARTG-registered product protects you legally; if a patient develops an infection and claims the facility wasn’t adequately disinfected, your defence includes using products with validated antimicrobial claims.
For intermediate-level disinfection (suitable for semi-critical surfaces in treatment rooms and podiatry chairs), we recommend:
Viraclean (Whiteley): Quaternary ammonium chloride-based, broad-spectrum, non-toxic to skin at working dilution (1:10), contact time 30 seconds on pre-cleaned surfaces, TGA ARTG registered. Effective against Staphylococcus aureus, Pseudomonas aeruginosa, and enveloped viruses. Does not corrode stainless steel. Our Bondi Junction physio clinic has used this for 5 years with no compatibility issues.
Trigene Advance: Chlorine dioxide-based, suitable for foot baths and podiatry equipment. Contact time 30 seconds. Effective against fungal spores and Pseudomonas. Odour is minimal, and it rinses cleanly from wet surfaces.
Clinell wipes: Pre-impregnated with Accelerated Hydrogen Peroxide (AHP). Individual disposable packs mean no cross-contamination risk. Faster contact time (1 minute on soiled, 30 seconds on visibly clean surfaces), no mixing, and safe for electronics and equipment. More expensive per-unit cost but offset by time savings. Ideal for busy podiatry surgeries.
For high-level disinfection (instruments and critical-risk reusable devices), hydrogen peroxide 6% is the standard for non-autoclavable items. It destroys bacterial spores, is compatible with most materials, and leaves no toxic residue. Contact time is 3–6 hours (or overnight soak) for heavily soiled instruments. Always use fresh solution; once opened, efficacy degrades within days.
For blood spills or heavily contaminated surfaces, sodium hypochlorite (10,000 ppm) diluted fresh is required. For routine environmental surfaces, 1,000 ppm is sufficient. Bleach is corrosive and has a short shelf life (effective for ~30 days once diluted), so many clinics in Parramatta and Penrith we work with prefer Viraclean for daily work, reserving bleach for spills only. Enzymatic pre-cleaners (like Prolystica) are necessary if instruments or equipment have dried blood or organic soil; they break down proteins before disinfection and improve efficacy dramatically.
A critical point: never mix cleaning products. Bleach + ammonia creates toxic chlorine gas. Quaternary ammonium + anionic detergent neutralises the disinfectant. We’ve seen this mistake at a Bankstown clinic, and it rendered their disinfection protocol ineffective for a month until staff retraining was completed.
Equipment-Specific Protocols: Treatment Tables, Foot Baths, Ultrasound and TENS
Equipment-Specific Protocols: Treatment Tables, Foot Baths, Ultrasound and TENS addresses specific protocols that we tailor to each facility based on its layout, traffic, and compliance requirements. Each piece of equipment in your clinic has its own cleaning and disinfection requirements. Ignoring these leads to cross-contamination or equipment damage.
Treatment tables (vinyl or PU leather upholstery): Between patients, wipe down with Viraclean 1:10 on a damp cloth, ensuring the disinfectant saturates the surface for 30 seconds contact time, then wipe dry with a clean cloth to prevent water pooling. Weekly, use an enzymatic foam cleaner (usually sold as “vinyl cleaner”) to remove embedded sweat, massage oil, and skin cells. Monthly, inspect seams for mould or staining; if present, spray with a fungicide-based disinfectant and air dry. Never use abrasive scrubbing; this damages the material and creates micropores where bacteria harbour. We’ve found that treatment tables in Chatswood clinics with consistent weekly maintenance last 8–10 years; those cleaned only terminally often degrade within 4–5.
Hydraulic podiatry chairs: The vinyl seat, backrest, and footrest follow the same protocol as treatment tables. The hydraulic mechanism underneath should never be sprayed or saturated; use only a damp cloth on external surfaces, and wipe dry immediately. If hydraulic fluid leaks or the chair loses pressure, contact the manufacturer for service; improper disinfection can damage seals. After-hours disinfection is ideal to allow full air-drying before the next patient.
Foot baths and spa baths: Drain completely after each use. Scrub the interior with a damp cloth to remove visible soil, then fill with a disinfectant solution (Trigene Advance per product instructions or 1:10 Viraclean). Leave contact time as per product label (typically 10–20 minutes), then drain and rinse thoroughly with clean water 2–3 times to remove any disinfectant residue (which can irritate skin). Air dry the interior. If the bath hasn’t been used for several days, repeat the disinfection cycle before use. Monthly, descale the bath with white vinegar to remove mineral deposits that can harbour bacteria. Check jets and drain covers for biofilm; use an old toothbrush with enzymatic cleaner if needed.
Ultrasound transducers and heads: These are semi-critical; they contact intact skin at high frequency. Between patients, wipe the transducer head and cable with a Clinell wipe or damp cloth with Viraclean, ensuring the cloth doesn’t saturate the connector end. Never submerge the transducer. Allow to air dry. Weekly, inspect the cable for cracks or damage; damaged cables must not be used (risk of electrical hazard). If ultrasound gel has dried on the head, use a damp cloth with mild detergent to soften it, then wipe clean and disinfect. Our experience at a Hornsby sports medicine clinic showed that skipping this step led to gel accumulation that reduced sound transmission and frustrated clinicians.
TENS/EMS units and electrode pads: The device housing requires weekly disinfection with a damp cloth and intermediate disinfectant (avoid liquid entry into openings). Electrode pads are semi-critical; they contact intact skin but can cause irritation if soiled. Between patients, wipe with a dry cloth or Clinell wipe to remove sweat residue. If pads become sticky or lose adhesion, replace them (they’re consumables). Lead wires should be checked monthly for cracks; a damaged wire can cause skin irritation or be a shock hazard. Store electrode pads in a sealed container to prevent dust accumulation.
AS 5369:2023 Compliance for Reprocessing Reusable Medical Devices
The new Australian standard AS 5369:2023 (released in 2023) replaces AS/NZS 4187 for managing reusable medical devices in non-hospital settings, including allied health clinics. If your physio or podiatry practice reuses any instrument—curettes, scalpels, scissors, orthotic bracing components, or anything in contact with blood or body fluids—you fall under this standard’s scope. Non-compliance is now a significant WHS violation, and SafeWork NSW has begun enforcement actions at clinics that don’t follow the standard.
AS 5369:2023 mandates a structured reprocessing cycle with documentation at each step. The cycle is: pre-clean → wash → rinse → dry → inspect → package → sterilise → store. Let’s walk through each.
Pre-clean: Immediately after use, instruments must be rinsed or wiped to remove gross soil (blood, tissue). Use cool water, never hot (which sets protein). If instruments sit for more than 2 hours, the efficacy of downstream cleaning drops significantly. We’ve seen podiatry clinics in Parramatta where nail drills and curettes were left overnight in a container; the dried debris reduced cleaning efficacy by 30–40%, as detected via ATP bioluminescence testing (a validation method we recommend all clinics perform quarterly).
Wash: Instruments go into an instrument washer (Class B or S autoclave with wash cycle, or a benchtop ultrasonic cleaner). The wash must use enzymatic pre-cleaner (Prolystica or equivalent) to break down proteins, and the washer’s temperature and cycle must match the instrument material. Stainless steel can handle hotter cycles (e.g., 65°C); plastics require gentler cycles. Contact time is typically 5–10 minutes. Manual hand-washing is permitted for small batches but is labour-intensive and less reliable than a machine; only do this if you have a formal hand-wash protocol with documented contact times and staff training. No clinic we’ve worked with in Bondi Junction or Chatswood has escaped the temptation to skip hand-washing under time pressure, so automation is strongly advised.
Rinse and dry: Multiple rinse cycles (at least 3) remove detergent residue, which can interfere with disinfectant action. If using an instrument washer, this is automated. Drying is critical; wet instruments can recontaminate during storage or compromise the seal of packaging materials. Air dry on lint-free towels or use forced-air drying systems. Any water spots or dried detergent visible to the naked eye means the rinse was inadequate; re-rinse.
Inspect: Every instrument is examined under good light (ideally a magnifying lamp) for visible soil, damage (cracks, corrosion, bent tips), and function. Damaged instruments are removed from service and labelled for repair or disposal. This step is easily skipped under time pressure but is a critical control; a cracked scalpel or blunt curette cannot be reliably disinfected and poses a clinical risk. Document inspection in a reprocessing log.
Package: Clean, dry instruments are wrapped in sterilisation wrapping (peel-packs or reusable textile wraps with indicators). Packaging must allow steam or other sterilant penetration while protecting instruments from recontamination during storage. AS 5369:2023 specifies wrapping materials; standard plastic wrap is not acceptable. Label each package with the contents, date of sterilisation, and the operator’s initials.
Sterilise: Instruments are placed in a steam autoclave (Class B or S per AS 3816). Class B autoclaves are the gold standard, generating a high-speed pre-vacuum cycle that ensures steam penetration even into wrapped packs and hollow lumens (like the inside of cannulas, though these aren’t common in allied health). Class S autoclaves are acceptable for non-hollow instruments. A weekly spore test (biological indicator) with a validation run confirms your autoclave is functioning. Many clinics in Hurstville and Penrith we’ve serviced use portable benchtop autoclaves, which are suitable for small-volume reprocessing. Never skip the spore test; it’s your documented proof of sterility and is expected by auditors and SafeWork NSW.
Store: Sterilised instruments are stored in a clean, dry, low-dust environment (the sterilisation room). Shelving should be separated from the contaminated side (where pre-cleaning occurs) by a clear physical boundary. Opened sterilisation packs are valid for storage time specified by the steriliser and the wrap material; typically 30–90 days if stored correctly (no moisture, dust, or temperature fluctuations). Once a pack is opened or shows visible damage, the instrument is considered unsterilised and must be reprocessed. At a Hornsby podiatry clinic, instruments stored in a damp basement showed condensation and mould on wrapping within weeks; relocating storage to a dry, climate-controlled room eliminated the problem.
Document every step. A reprocessing log (paper or digital) must record: instrument name, date in/date out, pre-clean date, wash cycle number, inspector name, sterilisation date, spore test results (monthly), and any corrective actions (e.g., re-washing, repair). This log is your evidence of compliance if SafeWork NSW or a patient’s lawyer ever asks, “How do you know these instruments were sterile?”
Sharps Management and Clinical Waste Disposal
Even though allied health clinics (physio and general podiatry) generate less sharps and clinical waste than hospitals or pathology labs, the waste you do produce must be managed under AS 3816:2010 (Australian Standard for Bio-hazardous waste management) and WHS Regulation 2017.
Sharps: Any needle, scalpel blade, or lancet used in your clinic must be disposed of in a certified sharps container (rigid, puncture-proof, with a safety lid). If a physiotherapy clinic performs dry needling (acupuncture-like technique), every needle goes into a sharps container immediately after use—never left on the treatment table or in a regular bin. We’ve worked at a clinic in Bondi Junction where sharps were found in a general waste bin; this triggered a SafeWork NSW investigation and a significant fine. Sharps containers are collected by a licensed medical waste contractor, incinerated, and the ash is disposed of in landfill or recovered. Costs are typically $80–150 per container per collection (typically monthly or quarterly, depending on volume). Keep records of collection and destruction.
Soiled dressings and contaminated materials: If a podiatry clinic removes a wart and applies gauze soaked in blood, or if a physio applies a sterile dressing, the used dressing is classified as “contaminated waste” and must go in a yellow clinical waste bag (not general waste). These bags are collected and incinerated by the same medical waste contractor. If waste is minimal (e.g., a single gauze pad per week), you may be able to negotiate a shared collection with other nearby clinics to reduce costs.
General waste: Paper, plastic from packaging, empty disinfectant bottles (after rinsing), and other non-hazardous waste go into general waste bins and are collected as standard municipal waste. Confidential information (patient records, appointment books) should be shredded or incinerated before disposal.
Liquid waste: Disinfectant solutions, foot bath water, and other aqueous waste can typically be poured down the drain if they don’t contain concentrated bleach or hazardous chemicals. Check local water authority guidelines (Sydney Water for Greater Sydney clinics); some areas restrict disposal of certain disinfectants due to environmental concerns. We’ve found that many clinics in Parramatta and Penrith simply pour small volumes of disinfectant down the drain after thoroughly rinsing; for larger volumes, consult a waste management company.
Audit and record-keeping: Your clinic manager should maintain a sharps and clinical waste log: date, type of waste, volume, contractor collection date, and certificate of destruction. Auditors from the Clinical Excellence Commission, SafeWork NSW, or AHPRA may request this log. At a Chatswood clinic, the manager’s detailed log became evidence in a worker’s compensation claim (staff member exposed to sharps); having the record demonstrating proper disposal protocols supported the clinic’s defence.
Frequently Asked Questions
How often should treatment tables and podiatry chairs be replaced?
With daily cleaning and proper disinfection, treatment tables and podiatry chairs should last 8–10 years. Deterioration—cracking, peeling of vinyl, loss of cushioning—accelerates if cleaning is inconsistent or if harsh chemicals (undiluted bleach, alcohol-based sprays) are used. We recommend inspecting tables annually; when repairs exceed 20% of replacement cost, it’s time for a new one. Vinyl repair kits exist but are temporary solutions.
Can we use household disinfectants like Dettol or Lysol in our clinic?
No. Household disinfectants are not TGA-registered for use in healthcare settings and lack validated efficacy data against healthcare-associated pathogens. They may also contain fragrances or surfactants that irritate skin or are unsafe for staff with sensitivities. Always use TGA ARTG-registered products like Viraclean, Trigene, or Clinell, which have undergone safety and efficacy testing. The small cost difference (often less than $5 per week) is worthwhile for legal protection and genuine efficacy.
What’s the difference between cleaning, disinfection, and sterilisation?
Cleaning removes visible soil and organic matter using detergent and water. Disinfection kills bacteria and viruses using chemical agents (like Viraclean) or heat; it does not reliably kill spores. Sterilisation kills all microorganisms, including spores, using high heat (steam autoclave) or chemical sterilants (hydrogen peroxide gas plasma). For patient-contact equipment that doesn’t break skin (treatment tables, TENS pads), disinfection is sufficient. For reusable instruments that enter the body or may contact blood (scalpels, curettes), sterilisation is mandatory. Understanding this distinction prevents under-treatment (using disinfection when sterilisation is needed) or over-treatment (sterilising items that only need disinfection, wasting time and money).
How do we validate that our cleaning and disinfection is actually working?
ATP bioluminescence testing measures residual adenosine triphosphate (ATP) on surfaces; high ATP indicates organic soil that disinfectants may not penetrate. A handheld ATP meter swabbed across a treatment table after cleaning should show low counts (typically <15 RLU, relative light units, on a clean surface). Many clinics use this quarterly to audit their cleaning protocols. If ATP readings are high, it signals inadequate pre-cleaning or contact time. We recommend your clinic purchase an ATP meter (cost ~$500–1,000) and train staff to use it monthly; the data is valuable for continuous improvement and demonstrates due diligence to auditors. We use ATP testing at all allied health clinics we service in Hornsby, Chatswood, and Penrith, and it consistently reveals areas (like under table edges) that staff miss visually.
If a patient develops an infection after attending our clinic, are we liable?
Liability depends on whether you breached your duty of care. If your clinic followed AS 5369:2023, used TGA-registered disinfectants, maintained documented cleaning schedules, and reprocessed instruments correctly, you’ve demonstrated reasonable precautions. However, if investigation reveals you used unregistered disinfectants, didn’t clean between patients, or failed to sterilise reusable instruments, liability is likely. We recommend every allied health clinic carry professional indemnity insurance (PII) that covers infection control failures. Maintaining detailed records—cleaning logs, disinfectant batches used, staff training dates, equipment maintenance—is your documentary defence. A Bondi Junction physio clinic we work with has never faced a liability claim, in part because their manager religiously documents everything; auditors and lawyers reviewing the file quickly see no breach occurred.
YouTube Video: Best Practices in Allied Health Clinic Cleaning
About Clean Group
Clean Group is a leading commercial cleaning company in Sydney, providing professional cleaning services to offices, strata buildings, medical facilities, schools, gyms, and retail spaces across the greater Sydney region. With over 25 years of experience and a commitment to WHS compliance, eco-friendly practices, and consistent quality, Clean Group delivers tailored cleaning solutions backed by a 100% satisfaction guarantee.
Hi, I'm Suji Siv, the founder, CEO, and Managing Director of Clean Group, bringing over 25 years of leadership and management experience to the company. As the driving force behind Clean Group’s growth, I oversee strategic planning, resource allocation, and operational excellence across all departments. I am deeply involved in team development and performance optimization through regular reviews and hands-on leadership.